

Intravenous iron in patients with heart failure and iron deficiency: an updated meta-analysis
- PMID: 36823953
- PMCID: PMC10946839
- DOI: 10.1002/ejhf.2810
Intravenous iron in patients with heart failure and iron deficiency: an updated meta-analysis
Abstract
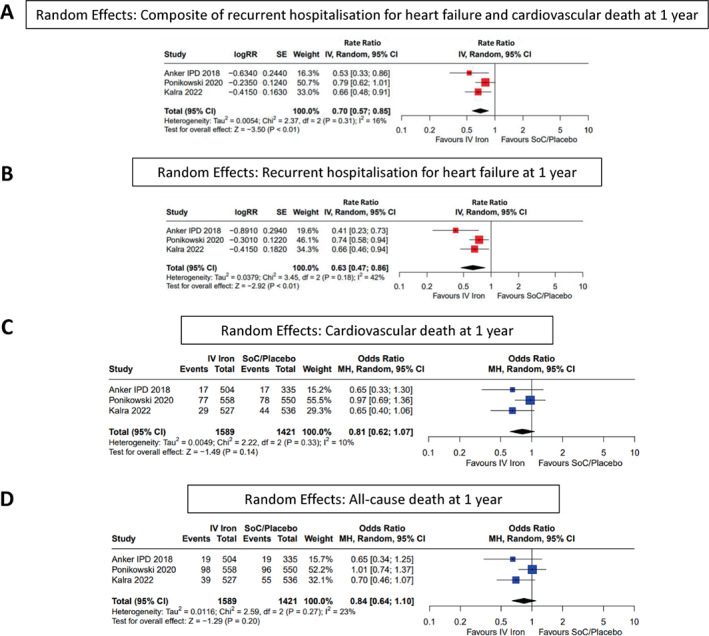
Aims: For patients with heart failure (HF) and iron deficiency (ID), randomized trials suggest that intravenous (IV) iron reduces hospitalizations for heart failure (HHF), but uncertainty exists about the effects in subgroups and the impact on mortality. We conducted a meta-analysis of randomized trials investigating the effect of IV iron on clinical outcomes in patients with HF.
Methods and results: We identified randomized trials published between 1 January 2000 and 5 November 2022 investigating the effect of IV iron versus standard care/placebo in patients with HF and ID in any clinical setting, regardless of HF phenotype. Trials of oral iron or not in English were not included. The main outcomes of interest were a composite of HHF and cardiovascular death (CVD), on HHF alone and on cardiovascular and all-cause mortality. Ten trials were identified with 3373 participants, of whom 1759 were assigned to IV iron. IV iron reduced the composite of recurrent HHF and CVD (rate ratio 0.75, 95% confidence interval [CI] 0.61-0.93; p < 0.01) and first HHF or CVD (odds ratio [OR] 0.72, 95% CI 0.53-0.99; p = 0.04). Effects on cardiovascular (OR 0.86, 95% CI 0.70-1.05; p = 0.14) and all-cause mortality (OR 0.93, 95% CI 0.78-1.12; p = 0.47) were inconclusive. Results were similar in analyses confined to the first year of follow-up, which was less disrupted by the COVID-19 pandemic. Subgroup analyses found little evidence of heterogeneity for the effect on the primary endpoint, although patients with transferrin saturation <20% (OR 0.67, 95% CI 0.49-0.92) may have benefited more than those with values ≥20% (OR 0.99, 95% CI 0.74-1.30) (heterogeneity p = 0.07).
Conclusion: In patients with HF and ID, this meta-analysis suggests that IV iron reduces the risk of HHF but whether this is associated with a reduction in cardiovascular or all-cause mortality remains inconclusive.
Keywords: Heart failure; IRONMAN; Intravenous iron; Iron deficiency; Meta-analysis.
© 2023 The Authors. European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures





Comment in
-
Benefits of intravenous iron supplementation in patients with heart failure: mounting evidence and open questions.Eur J Heart Fail. 2023 Apr;25(4):538-540. doi: 10.1002/ejhf.2787. Epub 2023 Mar 8. Eur J Heart Fail. 2023. PMID: 36722375 No abstract available.
References
-
- Masini G, Graham FJ, Pellicori P, Cleland JGF, Cuthbert JJ, Kazmi S, et al. Criteria for iron deficiency in patients with heart failure. J Am Coll Cardiol. 2021;79:341–51. - PubMed
-
- Anker SD, Colet JC, Filippatos G, Willenheimer R, Dickstein K, Drexler H, et al.; FAIR‐HF Trial Investigators . Ferric carboxymaltose in patients with heart failure and iron deficiency. N Engl J Med. 2009;361:2436–48. - PubMed
-
- Ponikowski P, van Veldhuisen DJ, Comin‐Colet J, Ertl G, Komajda M, Mareev V, et al.; CONFIRM‐HF Investigators . Beneficial effects of long‐term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency. Eur Heart J. 2015;36:657–68. - PMC - PubMed
-
- Anker SD, Kirwan BA, van Veldhuisen DJ, Filippatos G, Comin‐Colet J, Ruschitzka F, et al. Effects of ferric carboxymaltose on hospitalisations and mortality rates in iron‐deficient heart failure patients: an individual patient data meta‐analysis. Eur J Heart Fail. 2018;20:125–33. - PubMed
-
- Klip IT, Comin‐Colet J, Voors AA, Ponikowski P, Enjuanes C, Banasiak W, et al. Iron deficiency in chronic heart failure: an international pooled analysis. Am Heart J. 2013;165:575–82. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
