

Hemodynamic management during off-pump coronary artery bypass surgery: a narrative review of proper targets for safe execution and troubleshooting
- PMID: 36824043
- PMCID: PMC10391074
- DOI: 10.4097/kja.23103
Hemodynamic management during off-pump coronary artery bypass surgery: a narrative review of proper targets for safe execution and troubleshooting
Abstract
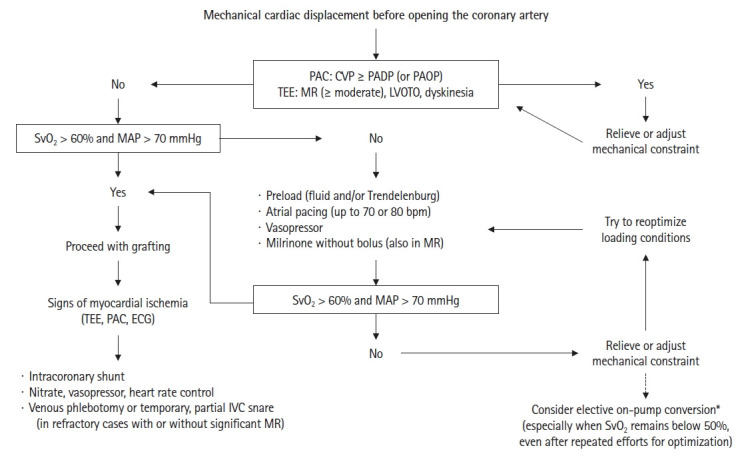
Off-pump coronary surgery requires mechanical cardiac displacement, which results in bi-ventricular systolic and diastolic dysfunction. Although transient, subsequent hemodynamic deterioration can be associated with poor prognosis and, in extreme cases, emergency conversion to on-pump surgery, which is associated with high morbidity and mortality. Thus, appropriate decision-making regarding whether the surgery can be proceeded based on objective hemodynamic targets is essential before coronary arteriotomy. For adequate hemodynamic management, avoiding myocardial oxygen supply-demand imbalance, which includes maintaining mean arterial pressure above 70 mmHg and preventing an increase in oxygen demand beyond the patient's coronary reserve, must be prioritized. Maintaining mixed venous oxygen saturation above 60%, which reflects the lower limit of adequate global oxygen supply-demand balance, is also essential. Above all, severe mechanical cardiac displacement incurring compressive syndromes, which cannot be overcome by adjusting major determinants of cardiac output, should be avoided. An uncompromising form of cardiac constraint can be ruled out as long as the central venous pressure is not equal to or greater than the pulmonary artery diastolic (or occlusion) pressure, as this would reflect tamponade physiology. In addition, transesophageal echocardiography should be conducted to rule out mechanical cardiac displacement-induced ventricular interdependence, dyskinesia, severe mitral regurgitation, and left ventricular outflow tract obstruction with or without systolic motion of the anterior leaflet of the mitral valve, which cannot be tolerated during grafting. Finally, the ascending aorta should be carefully inspected for gas bubbles to prevent hemodynamic collapse caused by a massive gas embolism obstructing the right coronary ostium.
Keywords: Cardiac tamponade; Hemodynamic monitoring; Mixed venous oxygen saturation; Off-pump coronary artery bypass; Swan-ganz catheterization; Transesophageal echocardiography..
Conflict of interest statement
Young Lan Kwak has been an editor in chief for the Korean Journal of Anesthesiology since 2016. However, she was not involved in any process of review for this article, including peer reviewer selection, evaluation, or decision-making. There were no other potential conflicts of interest relevant to this article.
Figures
Similar articles
-
Impact of transient decrease in mixed venous oxygen saturation on prognosis in off-pump coronary artery bypass surgery: a retrospective cohort study.Korean J Anesthesiol. 2023 Apr;76(2):107-115. doi: 10.4097/kja.22277. Epub 2022 Sep 7. Korean J Anesthesiol. 2023. PMID: 36068683 Free PMC article.
-
Hemodynamic changes during displacement of the beating heart using epicardial stabilization for off-pump coronary artery bypass graft surgery.J Cardiothorac Vasc Anesth. 2002 Dec;16(6):685-90. doi: 10.1053/jcan.2002.128418. J Cardiothorac Vasc Anesth. 2002. PMID: 12486647
-
Hemodynamic changes during posterior vessel off-pump coronary artery bypass: comparison between deep pericardial sutures and vacuum-assisted apical suction device.Ann Thorac Surg. 2004 Dec;78(6):2057-62. doi: 10.1016/j.athoracsur.2004.05.059. Ann Thorac Surg. 2004. PMID: 15561035 Clinical Trial.
-
Mechanisms of hemodynamic changes during off-pump coronary artery bypass surgery.Can J Anaesth. 2002 Oct;49(8):835-49. doi: 10.1007/BF03017418. Can J Anaesth. 2002. PMID: 12374714 Review.
-
Trans-esophageal echocardiography in off-pump coronary artery bypass grafting.Ann Card Anaesth. 2009 Jul-Dec;12(2):167. doi: 10.4103/0971-9784.53438. Ann Card Anaesth. 2009. PMID: 19602750 Review.
Cited by
-
Serum Periostin as a Novel Biomarker for Predicting 30-Day Major Adverse Cardiac Events After Off-Pump Coronary Artery Bypass Grafting.Ther Clin Risk Manag. 2025 Feb 18;21:161-176. doi: 10.2147/TCRM.S507435. eCollection 2025. Ther Clin Risk Manag. 2025. PMID: 39991461 Free PMC article.
-
Anesthesia for Minimally Invasive Coronary Artery Bypass Surgery.J Cardiovasc Dev Dis. 2025 Jun 18;12(6):232. doi: 10.3390/jcdd12060232. J Cardiovasc Dev Dis. 2025. PMID: 40558668 Free PMC article. Review.
References
-
- Puskas JD, Martin J, Cheng DC, Benussi S, Bonatti JO, Diegeler A, et al. ISMICS consensus conference and statements of randomized controlled trials of off-pump versus conventional coronary artery bypass surgery. Innovations (Phila) 2015;10:219–29. - PubMed
-
- Ueki C, Miyata H, Motomura N, Sakata R, Sakaguchi G, Akimoto T, et al. Off-pump technique reduces surgical mortality after elective coronary artery bypass grafting in patients with preoperative renal failure. J Thorac Cardiovasc Surg. 2018;156:976–83. - PubMed
-
- Keeling WB, Williams ML, Slaughter MS, Zhao Y, Puskas JD. Off-pump and on-pump coronary revascularization in patients with low ejection fraction: a report from the society of thoracic surgeons national database. Ann Thorac Surg. 2013;96:83–8. - PubMed
-
- Shroyer AL, Grover FL, Hattler B, Collins JF, McDonald GO, Kozora E, et al. On-pump versus off-pump coronary-artery bypass surgery. N Engl J Med. 2009;361:1827–37. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
