

Boosting of Waned Humoral and Cellular Responses to SARS-CoV-2 Variants of Concern Among Patients with Cancer
- PMID: 36824220
- PMCID: PMC7614214
- DOI: 10.1158/2767-9764.CRC-22-0298
Boosting of Waned Humoral and Cellular Responses to SARS-CoV-2 Variants of Concern Among Patients with Cancer
Abstract
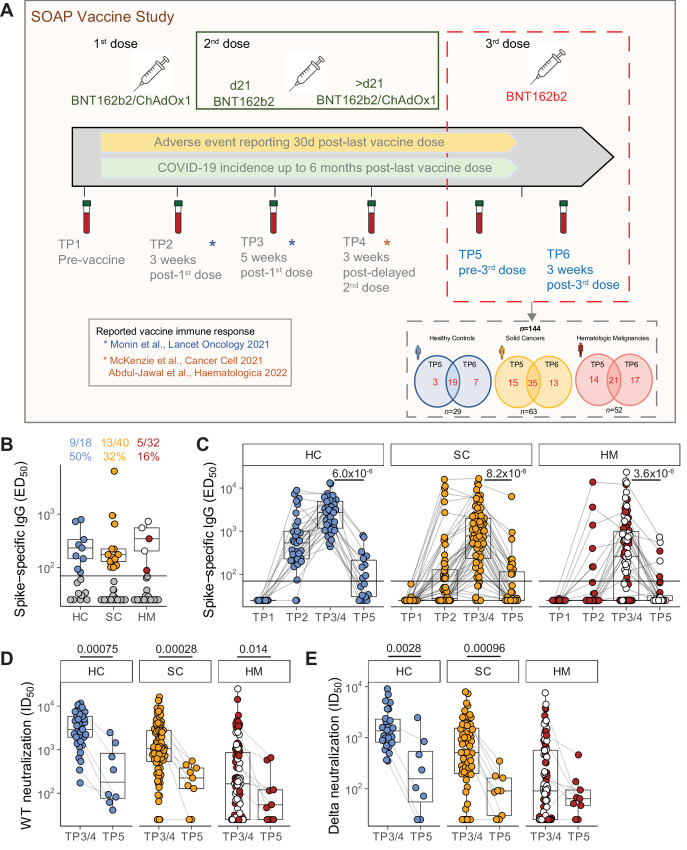
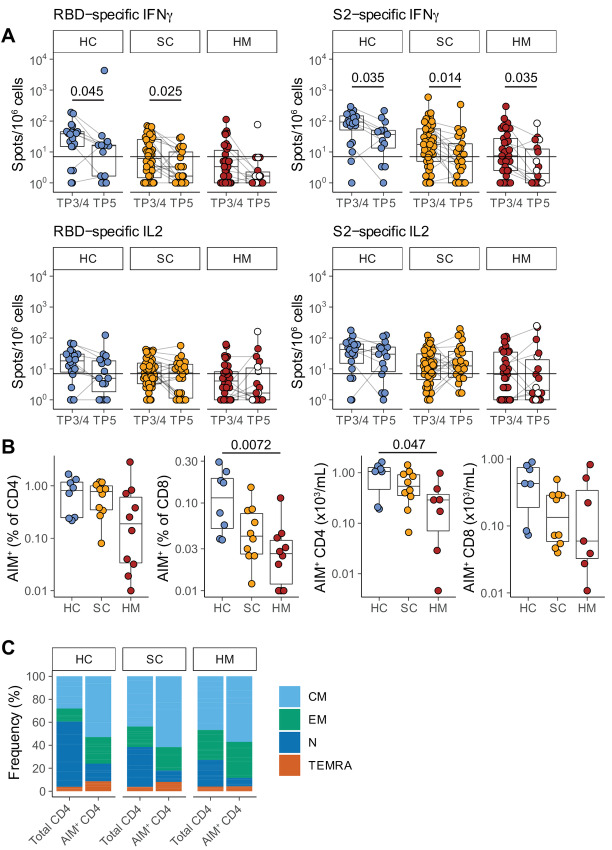
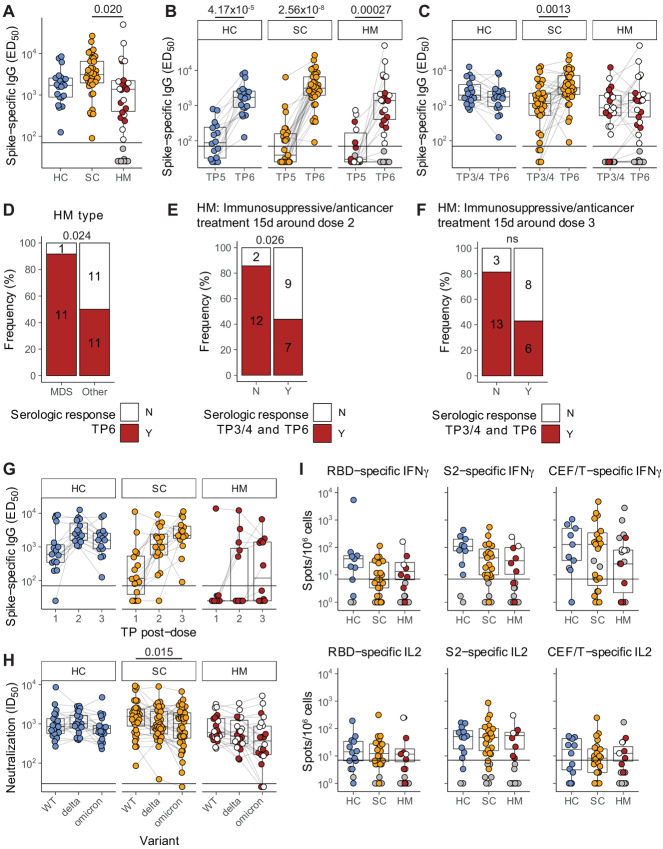
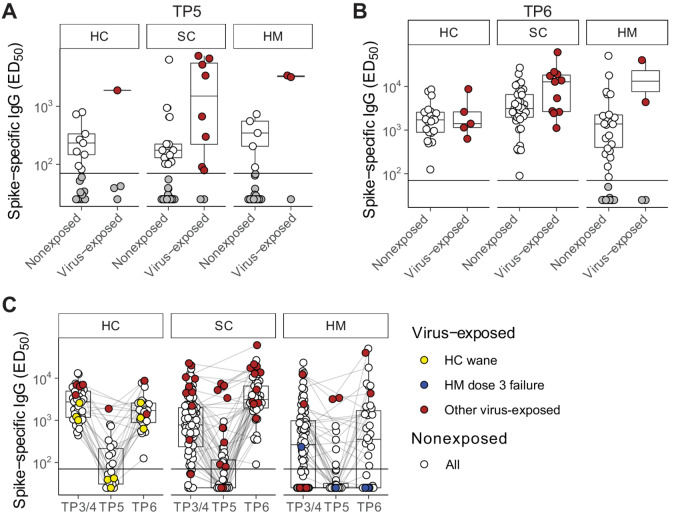
This study offers longitudinal insight into the impact of three SARS-CoV-2 vaccinations on humoral and cellular immunity in patients with solid cancers, patients with hematologic malignancies, and persons without cancer. For all cohorts, virus-neutralizing immunity was significantly depleted over a period of up to 9 months following the second vaccine dose, the one striking exception being IL2 production by SARS-CoV-2 antigen-specific T cells. Immunity was restored by the third vaccine dose, except in a substantial number of patients with hematologic malignancy, for whom both cancer type and treatment schedule were associated with nonresponse. Thus, whereas most patients with myelodysplastic syndrome were conspicuously good responders, some patients with other hematologic malignancies receiving cancer therapies within 2 weeks of vaccination showed no seroconversion despite three vaccine doses. Moreover, SARS-CoV-2 exposure during the course of the study neither prevented immunity waning, even in healthy controls, nor guaranteed vaccine responsiveness. These data offer real-world human immunologic insights that can inform health policy for patients with cancer.
Conflict of interest statement
Authors’ Disclosures P. Patten reports grants from Gilead, Roche; personal fees from Janssen, AstraZeneca, Abbvie, Beigene, and Novartis outside the submitted work. A.C. Hayday is co-founder, board member, and equity holder in ImmunoQure AG. This company is interested in antibodies but has no infectious disease or vaccine programs so cannot objectively be in conflict of interest with the work pursued in the study submitted to you; co-founder, board member, and equity holder in Gamma Delta Therapeutics. This company which no longer exists, was interested in gamma delta T cell which are an immunologic components, but the company has no infectious disease or vaccine programs so cannot objectively be in conflict of interest with the work pursued in the study submitted to you; co-founder, board member, and equity holder in Adaptate Biotherapeutics. This company, which no longer exists, was interested in gamma delta T cells which are an immunologic components, but the company has no infectious disease or vaccine programs so cannot objectively be in conflict of interest with the work pursued in the study submitted to you. A.C. Hayday receives research funding from Marengo Inc but this is a T-cell company with no vaccine program. A.C. Hayday receives research funding from Takeda Inc but this is funding solely relates to the use of gamma delta T cells for cancer immunotherapy. No disclosures were reported by the other authors.
Figures
References
-
- Monin L, Laing AG, Muñoz-Ruiz M, McKenzie DR, Del Molino Del Barrio I, Alaguthurai T, et al. . Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: interim analysis of a prospective observational study. Lancet Oncol 2021;22:765–78. - PMC - PubMed
-
- Immunisation TJCoVa; Green book chapter 14a. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploa....
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
