

Preschool-Aged Household Contacts as a Risk Factor for Viral Respiratory Infections in Healthcare Personnel
- PMID: 36824623
- PMCID: PMC9942663
- DOI: 10.1093/ofid/ofad057
Preschool-Aged Household Contacts as a Risk Factor for Viral Respiratory Infections in Healthcare Personnel
Abstract
Background: Viral respiratory infections (VRIs) are common and are occupational risks for healthcare personnel (HCP). VRIs can also be acquired at home and other settings among HCPs. We sought to determine if preschool-aged household contacts are a risk factor for VRIs among HCPs working in outpatient settings.
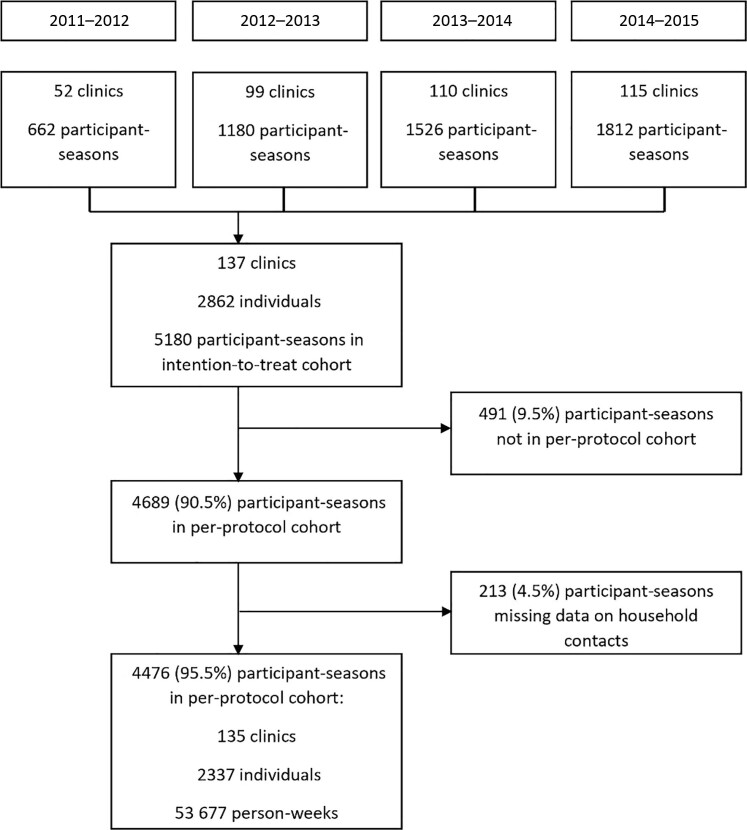
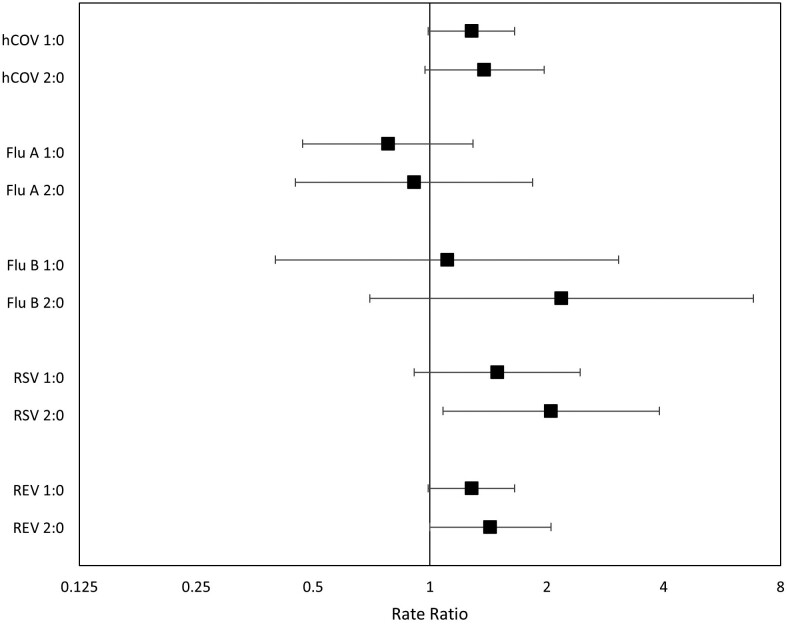
Methods: We conducted a secondary analysis of data from a cluster randomized trial at 7 medical centers in the United States over 4 influenza seasons from 2011-2012 to 2014-2015. Adult HCPs who routinely came within 6 feet of patients with respiratory infections were included. Participants were tested for respiratory viruses whenever symptomatic and at 2 random times each season when asymptomatic. The exposure of interest was the number of household contacts 0-5 years old (preschool-aged) at the beginning of each HCP-season. The primary outcome was the rate of polymerase chain reaction-detected VRIs, regardless of symptoms. The VRI incidence rate ratio (IRR) was calculated using a mixed-effects Poisson regression model that accounted for clustering at the clinic level.
Results: Among the 4476 HCP-seasons, most HCPs were female (85.4%) and between 30 and 49 years of age (54.6%). The overall VRI rate was 2.04 per 100 person-weeks. In the adjusted analysis, HCPs having 1 (IRR, 1.22 [95% confidence interval {CI}, 1.05-1.43]) and ≥2 (IRR, 1.35 [95% CI, 1.09-1.67]) preschool-aged household contacts had higher VRI rates than those with zero preschool-aged household contacts.
Conclusions: Preschool-aged household contacts are a risk factor for developing VRIs among HCPs working in outpatient settings.
Keywords: healthcare personnel; healthcare-associated infections; viral respiratory infections.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. All authors: No reported conflicts.
Figures

References
-
- Pappas DE, Hendley JO. The common cold and decongestant therapy. Pediatr Rev 2011; 32:47–54. - PubMed
-
- Bischoff WE, Swett K, Leng I, Peters TR. Exposure to influenza virus aerosols during routine patient care. J Infect Dis 2013; 207:1037–46. - PubMed
-
- Lindsley WG, Blachere FM, Davis KA, et al. . Distribution of airborne influenza virus and respiratory syncytial virus in an urgent care medical clinic. Clin Infect Dis 2010; 50:693–8. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
