

This is a preprint.
Sleep-Disordered Breathing Destabilizes Ventricular Repolarization
- PMID: 36824787
- PMCID: PMC9949208
- DOI: 10.1101/2023.02.10.23285789
Sleep-Disordered Breathing Destabilizes Ventricular Repolarization
Update in
-
Sleep-disordered breathing destabilizes ventricular repolarization: Cross-sectional, longitudinal, and experimental evidence.Heart Rhythm. 2025 Mar;22(3):808-816. doi: 10.1016/j.hrthm.2024.08.054. Epub 2024 Aug 28. Heart Rhythm. 2025. PMID: 39214391
Abstract
Rationale: Sleep-disordered breathing (SDB) increases the risk of cardiac arrhythmias and sudden cardiac death.
Objectives: To characterize the associations between SDB, intermittent hypoxemia, and the beat-to-beat QT variability index (QTVI), a measure of ventricular repolarization lability associated with a higher risk for cardiac arrhythmias, sudden cardiac death, and mortality.
Methods: Three distinct cohorts were used for the current study. The first cohort, used for cross-sectional analysis, was a matched sample of 122 participants with and without severe SDB. The second cohort, used for longitudinal analysis, consisted of a matched sample of 52 participants with and without incident SDB. The cross-sectional and longitudinal cohorts were selected from the Sleep Heart Health Study participants. The third cohort comprised 19 healthy adults exposed to acute intermittent hypoxia and ambient air on two separate days. Electrocardiographic measures were calculated from one-lead electrocardiograms.
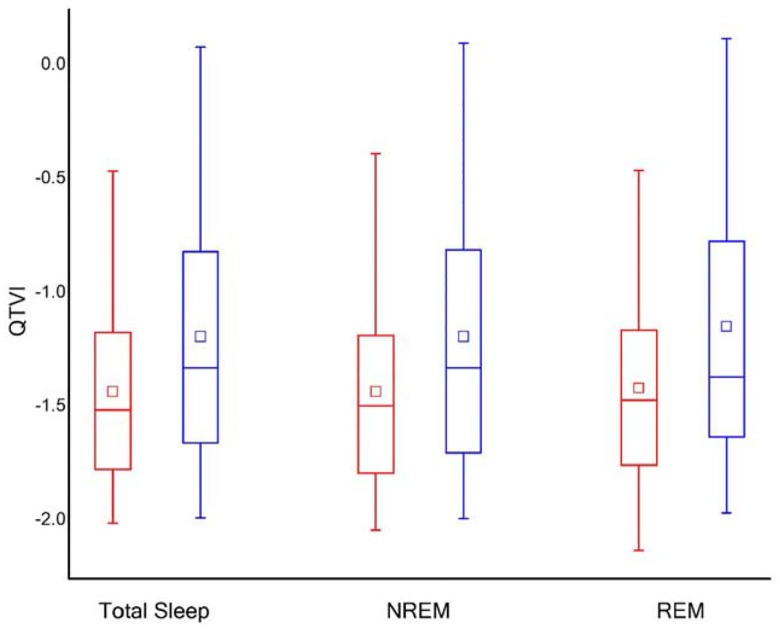
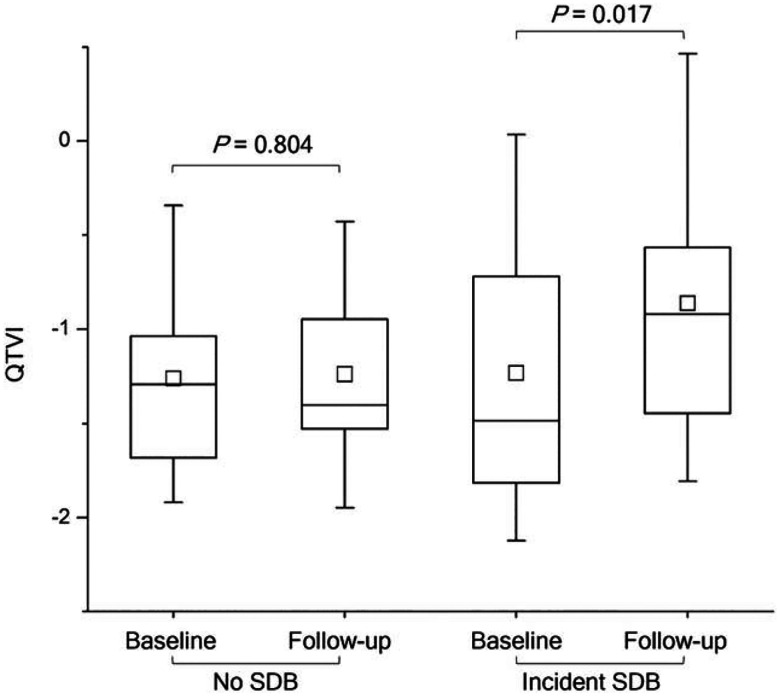
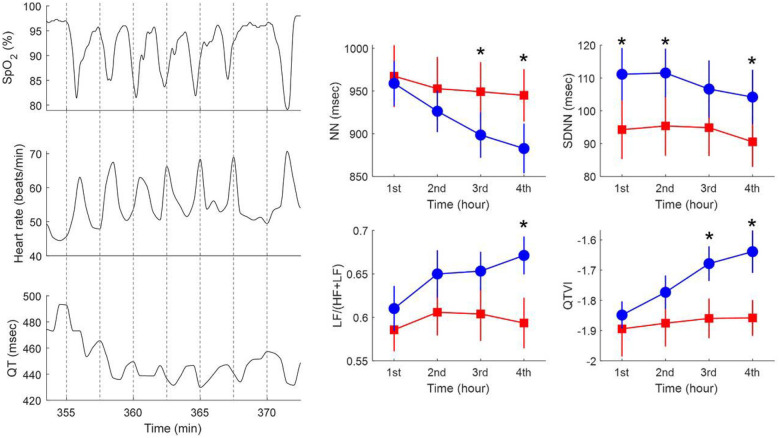
Results: Compared to those without SDB, participants with severe SDB had greater QTVI (-1.19 in participants with severe SDB vs. -1.43 in participants without SDB, P = 0.027), heart rate (68.34 vs. 64.92 beats/minute; P = 0.028), and hypoxemia burden during sleep as assessed by the total sleep time with oxygen saturation less than 90% (TST90; 11.39% vs. 1.32%, P < 0.001). TST90, but not the frequency of arousals, was a predictor of QTVI. QTVI during sleep was predictive of all-cause mortality. With incident SDB, mean QTVI increased from -1.23 to -0.86 over 5 years (P = 0.017). Finally, exposing healthy adults to acute intermittent hypoxia for four hours progressively increased QTVI (from -1.85 at baseline to -1.64 after four hours of intermittent hypoxia; P = 0.016).
Conclusions: Prevalent and incident SDB are associated with ventricular repolarization instability, which predisposes to ventricular arrhythmias and sudden cardiac death. Intermittent hypoxemia destabilizes ventricular repolarization and may contribute to increased mortality in SDB.
Keywords: Beat-to-beat QT variability index; QTVI; Sleep Heart Health Study; Sleep apnea; intermittent hypoxemia; intermittent hypoxia.
Figures
References
-
- Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, Hamilton GS, Dharmage SC. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med Rev 2017; 34: 70–81. - PubMed
-
- Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 2000; 342: 1378–1384. - PubMed
-
- Leung RS, Bradley TD. Sleep apnea and cardiovascular disease. Am J Respir Crit Care Med 2001; 164: 2147–2165. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources