

This is a preprint.
Genotype and Clinical Characteristics of Patients with Wolfram Syndrome and WFS1-related Disorders
- PMID: 36824811
- PMCID: PMC9949199
- DOI: 10.1101/2023.02.15.23284904
Genotype and Clinical Characteristics of Patients with Wolfram Syndrome and WFS1-related Disorders
Update in
-
Genotype and clinical characteristics of patients with Wolfram syndrome and WFS1-related disorders.Front Genet. 2023 Jun 21;14:1198171. doi: 10.3389/fgene.2023.1198171. eCollection 2023. Front Genet. 2023. PMID: 37415600 Free PMC article.
Abstract
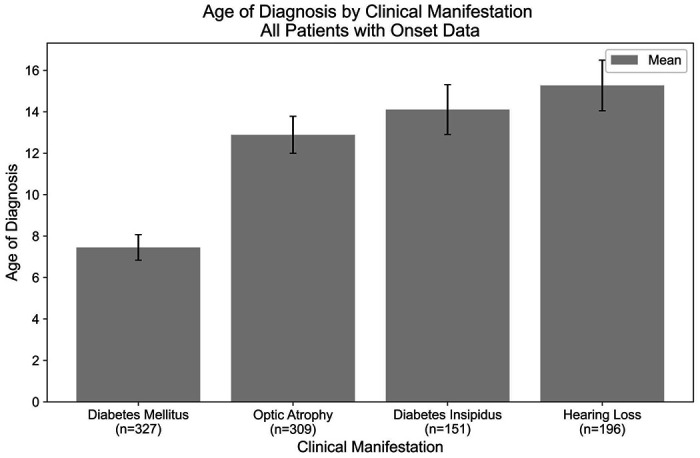
Objective: Wolfram syndrome (WFS) is an autosomal recessive disorder associated with juvenile-onset diabetes mellitus, optic atrophy, diabetes insipidus, and sensorineural hearing loss. We sought to elucidate the relationship between genotypic and phenotypic presentations of Wolfram syndrome which would assist clinicians in classifying the severity and prognosis of Wolfram syndrome more accurately.
Approach: Patient data from the Washington University International Registry and Clinical Study for Wolfram Syndrome and patient case reports were analyzed to select for patients with two recessive mutations in the WFS1 gene. Mutations were classified as being either nonsense/frameshift variants or missense/in-frame insertion/deletion variants and statistical analysis was performed using unpaired and paired t-tests and one- and two-way ANOVA with Tukey's or Dunnett's tests.
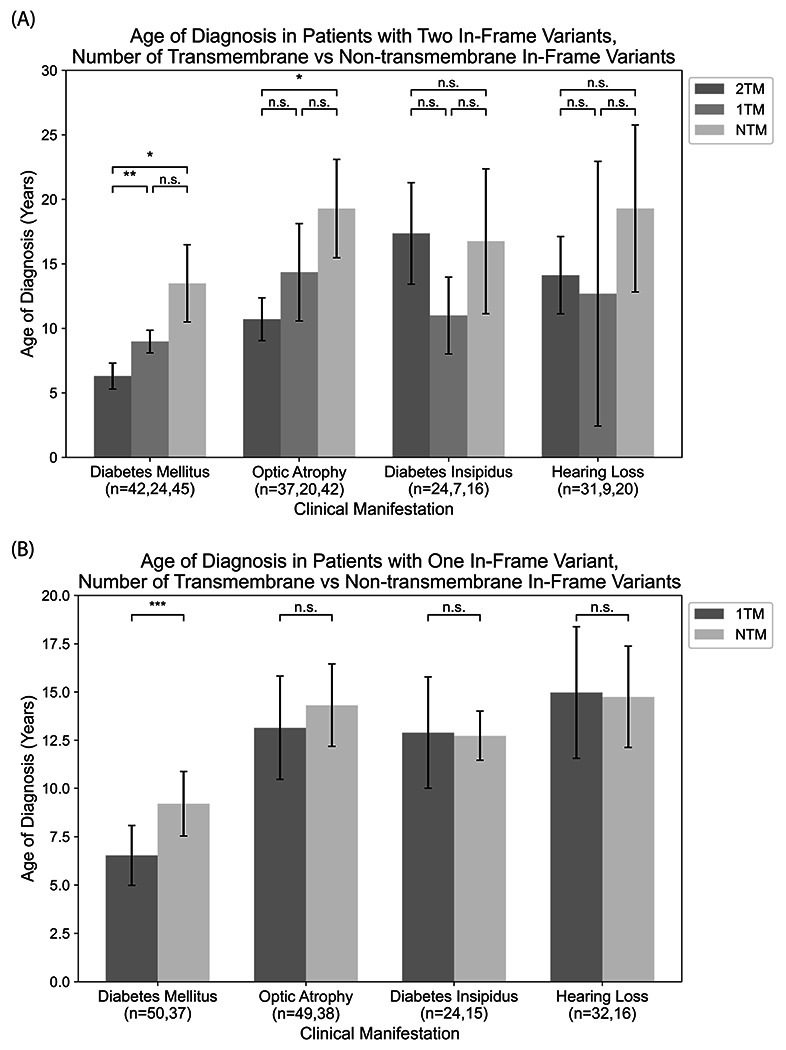
Results: A greater number of genotype variants correlated with earlier onset and a more severe presentation of Wolfram syndrome. Secondly, non-sense and frameshift variants had more severe phenotypic presentations than missense variants, as evidenced by optic atrophy emerging significantly earlier in patients with 2 nonsense/frameshift alleles compared with 0 missense transmembrane variants. In addition, the number of transmembrane in-frame variants demonstrated a statistically significant dose-effect on age of onset of diabetes mellitus and optic atrophy.
Summary / conclusions: The results contribute to our current understanding of the genotype-phenotype relationship of Wolfram syndrome, suggesting that alterations in coding sequences result in significant changes in the presentation and severity of Wolfram. The impact of these findings is significant, as the results will aid clinicians in predicting more accurate prognoses and pave the way for personalized treatments for Wolfram syndrome.
Conflict of interest statement
Conflict of Interest
FU is an inventor of three patents related to the treatment of Wolfram syndrome, US 9,891,231 SOLUBLE MANF IN PANCREATIC BETA CELL DISORDERS and US 10,441,574 and US 10,695,324 TREATMENT FOR WOLFRAM SYNDROME AND OTHER ER STRESS DISORDERS. FU is a Founder and President of CURE4WOLFRAM, INC. JRM is a consultant for Sana Biotechnology.
Figures

References
-
- Barrett T.G., Bundey S.E., and Macleod A.F., Neurodegeneration and diabetes: UK nationwide study of Wolfram (DIDMOAD) syndrome. The Lancet 346 (1995) 1458–1463. - PubMed
-
- de Heredia M.L., Cleries R., and Nunes V., Genotypic classification of patients with Wolfram syndrome: insights into the natural history of the disease and correlation with phenotype. Genet Med 15 (2013) 497–506. - PubMed