

Congenital lung abnormalities on magnetic resonance imaging: the CLAM study
- PMID: 36826502
- PMCID: PMC10290040
- DOI: 10.1007/s00330-023-09458-7
Congenital lung abnormalities on magnetic resonance imaging: the CLAM study
Abstract
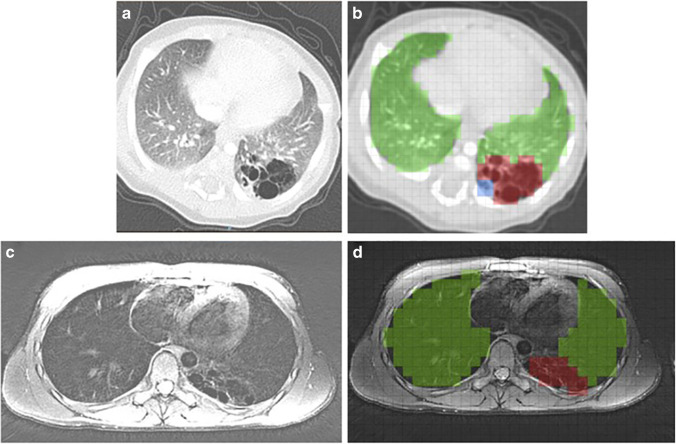
Objectives: Follow-up of congenital lung abnormalities (CLA) is currently done with chest computer tomography (CT). Major disadvantages of CT are exposure to ionizing radiation and need for contrast enhancement to visualise vascularisation. Chest magnetic resonance imaging (MRI) could be a safe alternative to image CLA without using contrast agents. The objective of this cohort study was to develop a non-contrast MRI protocol for the follow-up of paediatric CLA patients, and to compare findings on MRI to postnatal CT in school age CLA patients.
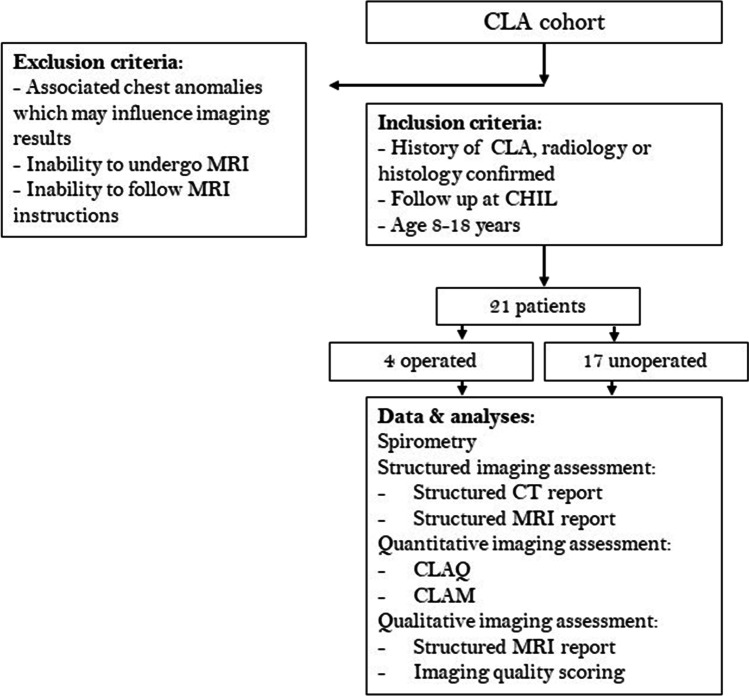
Methods: Twenty-one CLA patients, 4 after surgical resection and 17 unoperated (mean age 12.8 (range 9.4-15.9) years), underwent spirometry and chest MRI. MRI was compared to postnatal CT on appearance and size of the lesion, and lesion associated abnormalities, such as hyperinflation and atelectasis.
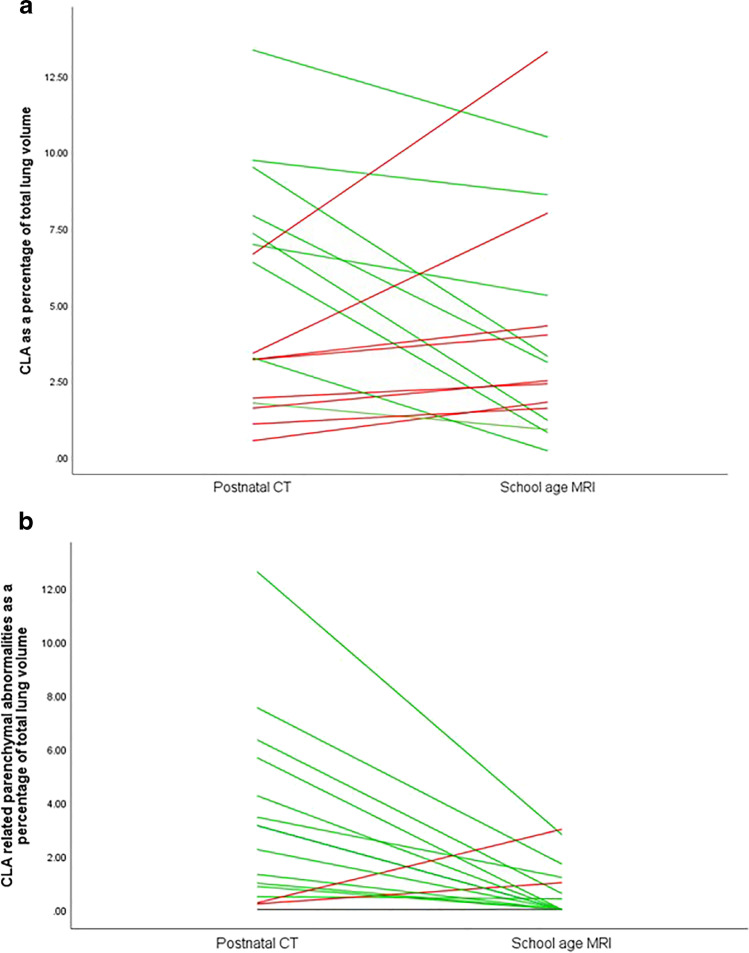
Results: By comparing school-age chest MRI to postnatal CT, radiological appearance and diagnostic interpretation of the type of lesion changed in 7 (41%) of the 17 unoperated patients. In unoperated patients, the relative size of the lesion in relation to the total lung volume remained stable (0.9% (range - 6.2 to + 6.7%), p = 0.3) and the relative size of lesion-associated parenchymal abnormalities decreased (- 2.2% (range - 0.8 to + 2.8%), p = 0.005).
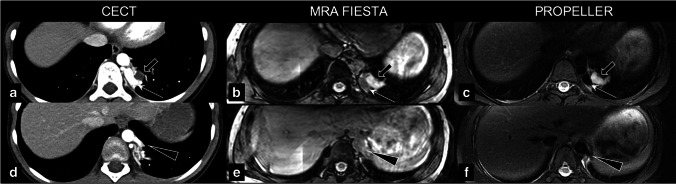
Conclusion: Non-contrast-enhanced chest MRI was able to identify all CLA-related lung abnormalities. Changes in radiological appearance between MRI and CT were related to CLA changes, patients' growth, and differences between imaging modalities. Further validation is needed for MRI to be introduced as a safe imaging method for the follow-up of paediatric CLA patients.
Key points: • Non-contrast-enhanced chest MRI is able to identify anatomical lung changes related to congenital lung abnormalities, including vascularisation. • At long-term follow-up, the average size of congenital lung abnormalities in relation to normal lung volume remains stable. • At long-term follow-up, the average size of congenital lung abnormalities associated parenchymal abnormalities such as atelectasis in relation to normal lung volume decreases.
Keywords: CT; Congenital lung abnormalities; Imaging; MRI; Paediatric.
© 2023. The Author(s).
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies:
H. Tiddens:
Novartis (partner in IMI project), Thirona (joint PPS grant), Vectura Group (unconditional grand for PhD research program), Insmed (consultant for clinical trial design), Novartis (Consultant), Thirona (consultant) and Vertex (faculty member for advance course).
P. Ciet:
Editamed (funding unrelated to submitted work).
Figures


References
-
- Hermelijn SM, Elders B, Ciet P, Wijnen RMH, Tiddens H, Schnater JM. A clinical guideline for structured assessment of CT-imaging in congenital lung abnormalities. Paediatr Respir Rev. 2021;37:80–88. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
