

Virtual Reality Simulator versus Conventional Advanced Life Support Training for Cardiopulmonary Resuscitation Post-Cardiac Surgery: A Randomized Controlled Trial
- PMID: 36826563
- PMCID: PMC9962457
- DOI: 10.3390/jcdd10020067
Virtual Reality Simulator versus Conventional Advanced Life Support Training for Cardiopulmonary Resuscitation Post-Cardiac Surgery: A Randomized Controlled Trial
Abstract
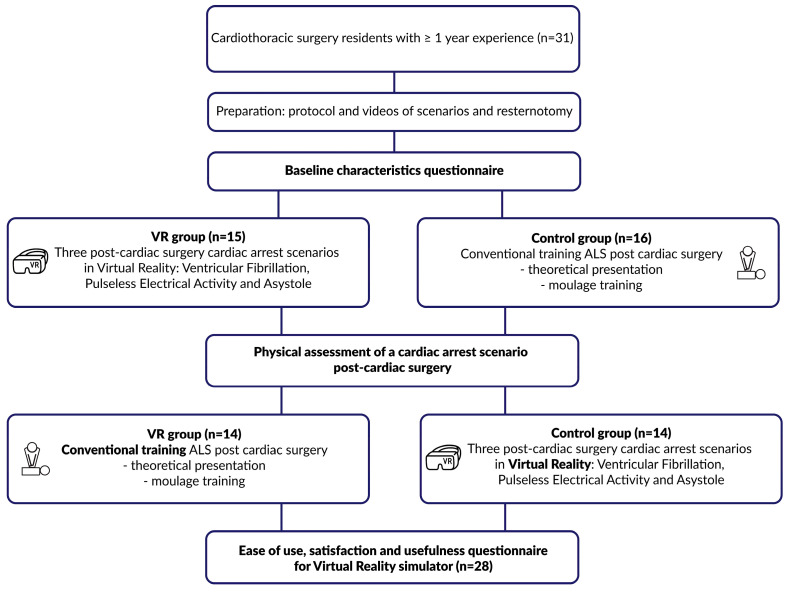
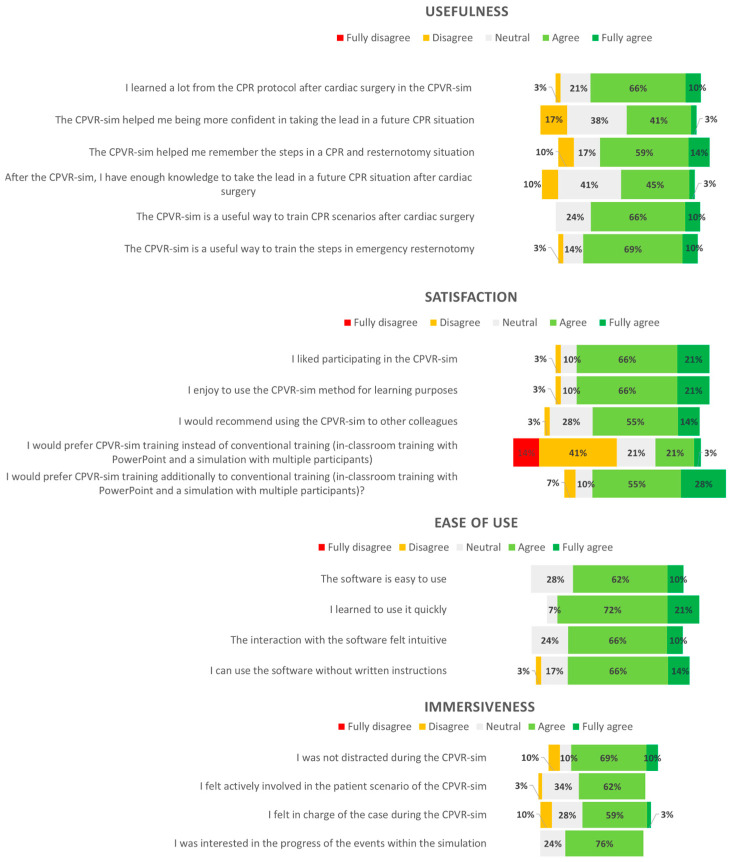
External chest compressions are often ineffective for patients arresting after cardiac surgery, for whom emergency resternotomy may be required. A single-blinded randomized controlled trial (RCT) was performed, with participants being randomized to a virtual reality (VR) Cardiac Surgical Unit Advanced Life Support (CSU-ALS) simulator training arm or a conventional classroom CSU-ALS training arm. Twenty-eight cardiothoracic surgery (CTS) residents were included and subsequently assessed in a moulage scenario in groups of two, either participating as a leader or surgeon. The primary binary outcomes were two time targets: (1) delivering three stacked shocks within 1 min and (2) resternotomy within 5 min. Secondary outcomes were the number of protocol mistakes made and a questionnaire after the VR simulator. The conventional training group administered stacked shocks within 1 min in 43% (n = 6) of cases, and none in the VR group reached this target, missing it by an average of 25 s. The resternotomy time target was reached in 100% of the cases (n = 14) in the conventional training group and in 83% of the cases (n = 10) in the VR group. The VR group made 11 mistakes in total versus 15 for those who underwent conventional training. Participants reported that the VR simulator was useful and easy to use. The results show that the VR simulator can provide adequate CSU-ALS training. Moreover, VR training results in fewer mistakes suggesting that repetitive practice in an immersive environment improves skills.
Keywords: cardiac surgery; cardiopulmonary resuscitation; emergency resternotomy; manikin training; medical training; simulation training; virtual reality; virtual reality simulation.
Conflict of interest statement
A.H.S., E.A.F.M., J.J.P., R.A.R., S.A.M. and W.B. are co-developers of the CPVR software.
Figures

References
-
- Lott C., Truhlář A., Alfonzo A., Barelli A., González-Salvado V., Hinkelbein J., Nolan J.P., Paal P., Perkins G.D., Thies K.C., et al. European Resuscitation Council Guidelines 2021: Cardiac Arrest in Special Circumstances. Resuscitation. 2021;161:152–219. doi: 10.1016/j.resuscitation.2021.02.011. - DOI - PubMed
-
- Dunning J., Levine A., Ley J., Strang T., Lizotte D.E., Lamarche Y., Bartley T., Zellinger M., Katz N., Arora R.C., et al. The Society of Thoracic Surgeons Expert Consensus for the Resuscitation of Patients Who Arrest After Cardiac Surgery. Ann. Thorac. Surg. 2017;103:1005–1020. doi: 10.1016/j.athoracsur.2016.10.033. - DOI - PubMed
-
- Greif R., Lockey A., Breckwoldt J., Carmona F., Conaghan P., Kuzovlev A., Pflanzl-Knizacek L., Sari F., Shammet S., Scapigliati A., et al. European Resuscitation Council Guidelines 2021: Education for Resuscitation. Resuscitation. 2021;161:388–407. doi: 10.1016/j.resuscitation.2021.02.016. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
