

Mechanical versus Bioprosthetic Aortic Valve Replacement in Middle-Aged Adults: A Systematic Review and Meta-Analysis
- PMID: 36826586
- PMCID: PMC9965629
- DOI: 10.3390/jcdd10020090
Mechanical versus Bioprosthetic Aortic Valve Replacement in Middle-Aged Adults: A Systematic Review and Meta-Analysis
Abstract
Background: Mechanical prostheses and bioprosthetic prostheses have their own advantages and disadvantages. Mechanical ones are recommended for younger patients (<50 years old), and bioprosthetic ones are recommended for older patients (>70 years old). There is still debate regarding which kind of prosthesis is better for middle-aged patients (50 to 70 years old) receiving aortic valve replacement (AVR). To solve this problem, we conducted this meta-analysis. Given that only one randomized controlled trial (RCT) study was included, we conducted a subgroup analysis of RCT and propensity score matching (PSM) retrospective studies to reduce the bias.
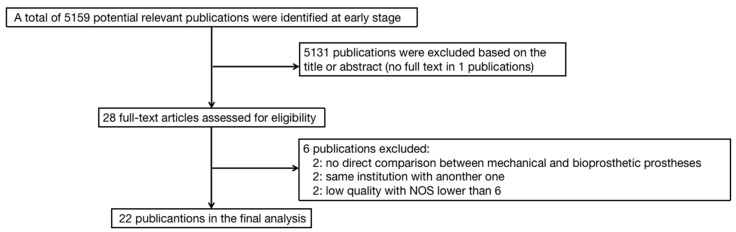
Methods: We systematically searched articles related to clinical outcomes of mechanical and bioprosthetic prostheses in middle-aged patients receiving AVR in the PubMed, Cochrane Library, and China National Knowledge Infrastructure (CNKI) databases. The published date was up to 1 October 2022. Studies were excluded if not only middle-aged patients were included, or if they lacked direct comparisons between mechanical and bioprosthetic prostheses.
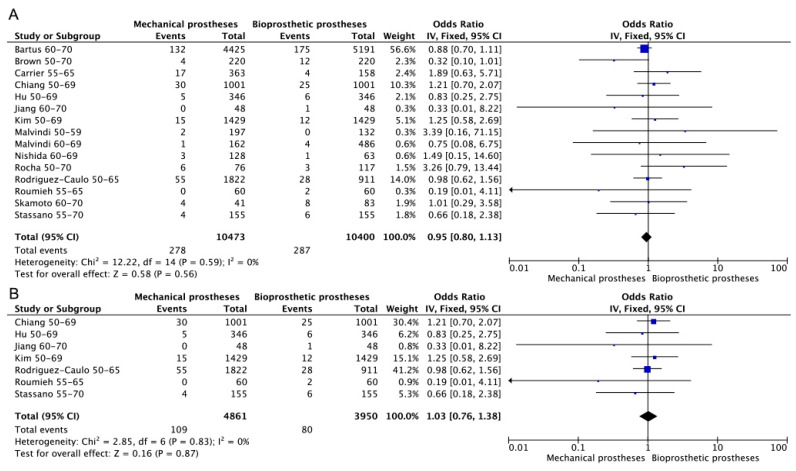
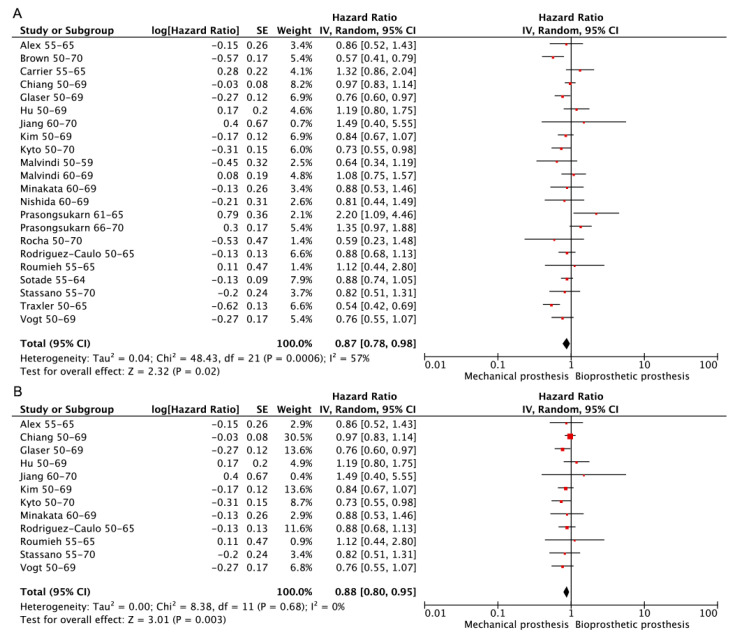
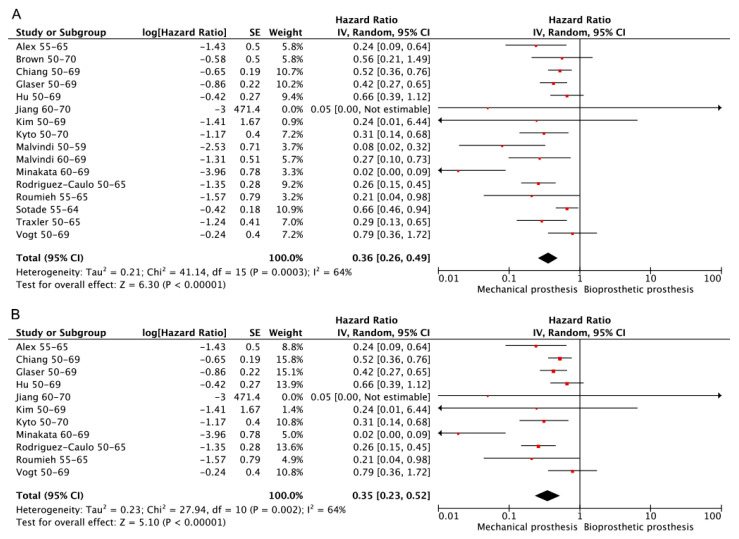
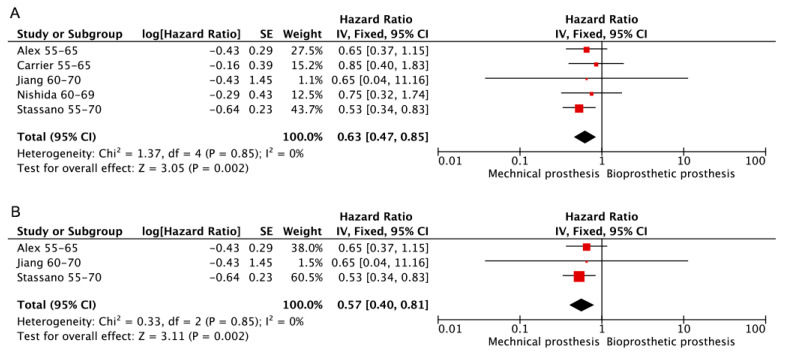
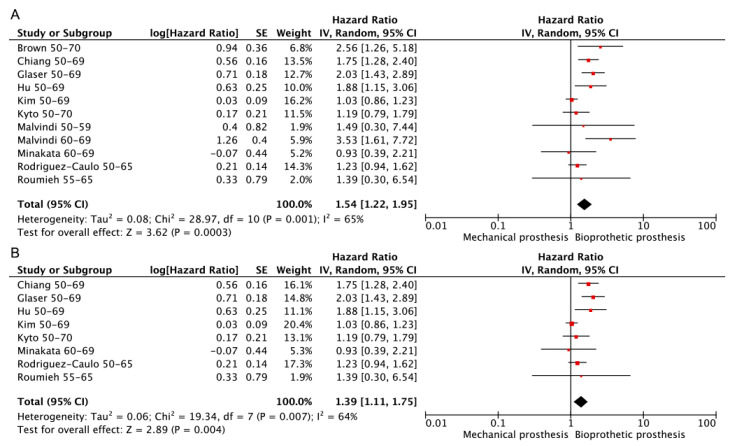
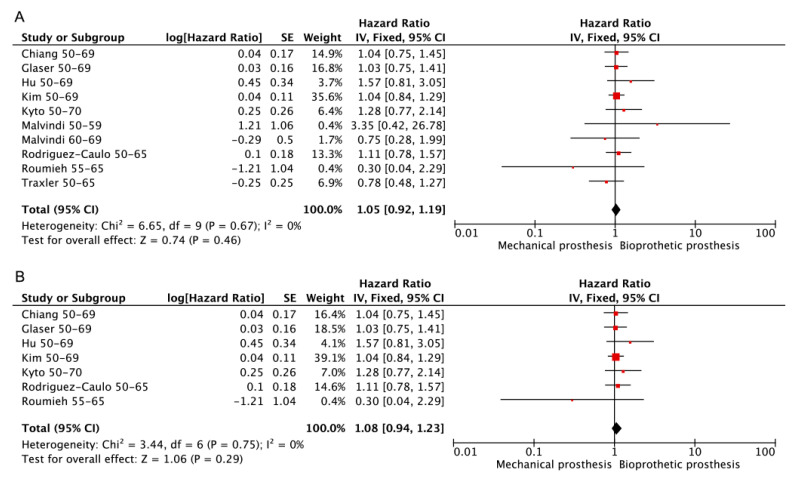
Results: In total, 22 studies with 32,298 patients were included in the final analysis. The results show that patients aged between 50 and 70 receiving AVR with mechanical prostheses achieved better long-term survival and fewer reoperations and valve-related events but suffered more with bleeding events. No significant difference could be found in terms of early mortality and long-term cardiac death. The same results could be observed in the subgroup analysis of RCT and PSM retrospective studies.
Conclusion: Both mechanical and bioprosthetic prostheses are beneficial to middle-aged patients undertaking AVR procedures. However, mechanical prostheses show better clinical outcomes in long-term survival and comorbidities. Individual recommendation is still necessary.
Keywords: bioprosthetic prostheses; clinical outcomes; mechanical prostheses; meta-analysis; middle-aged.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Vogt F., Santarpino G., Fujita B., Frerker C., Bauer T., Beckmann A., Bekeredjian R., Bleiziffer S., Möllmann H., Walther T., et al. GARY Executive Board. Surgical aortic valve replacement in patients aged 50–69 years-insights from the German Aortic Valve Registry (GARY) Eur. J. Cardiothorac. Surg. 2022;62:ezac286. doi: 10.1093/ejcts/ezac286. - DOI - PubMed
-
- Vahanian A., Beyersdorf F., Praz F., Milojevic M., Baldus S., Bauersachs J., Capodanno D., Conradi L., De Bonis M., De Paulis R., et al. ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022;43:561–632. doi: 10.1093/eurheartj/ehab395. - DOI - PubMed
-
- Nishimura R.A., Otto C.M., Bonow R.O., Carabello B.A., Erwin J.P., Fleisher L.A., Jneid H., Mack M.J., McLeod C.J., O’Gara P.T., et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2017;70:252–289. doi: 10.1016/j.jacc.2017.03.011. - DOI - PubMed
-
- Baumgartner H., Falk V., Bax J.J., De Bonis M., Hamm C., Holm P.J., Iung B., Lancellotti P., Lansac E., Rodriguez Muñoz D., et al. ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017;38:2739–2791. doi: 10.1093/eurheartj/ehx391. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
