

An algorithmic approach of reconstruction for cranioplasty failure: A case series
- PMID: 36827034
- PMCID: PMC11309693
- DOI: 10.1097/MD.0000000000033011
An algorithmic approach of reconstruction for cranioplasty failure: A case series
Abstract
Rationale: Cranioplasty is a surgical procedure used to repair cranial defects for both cosmetic and functional reasons. The complication rate of cranioplasty is between 10% and 50%. The failure of cranioplasty is associated with various factors, including etiologies, types of material, and the timing of cranioplasty. In this study, a case series of managing cranioplasty complications at a single institution.
Patient concerns: Eighteen patients were identified who underwent craniofacial defect reconstruction due to the failure of their initial cranioplasty between January 2010 and May 2020. Five men (27.78%) and thirteen women (72.22%) were included. The mean age was 39.61 years old. The average follow-up duration was 5.94 years.
Diagnoses: The indication for initial cranioplasty included previous decompressive craniectomy (77.78%, n = 14), traumatic cranial defects (16.67%, n = 3), and congenital cranial deformity (5.56%, n = 1). The reported complications were infection (50%, n = 9), implant exposure (50%, n = 9), wound dehiscence (22.22%, n = 4) and cranial deformity (11.11%, n = 2).
Interventions: More than half of the materials used for initial cranioplasty were synthetic [titanium mesh: 44.44%, n = 8; polymethyl metacrylate: 5.56%, n = 1; titanium mesh and polymethyl metacrylate: 5.56%, n = 1], while 44.44% of the patients received autologous bone graft.
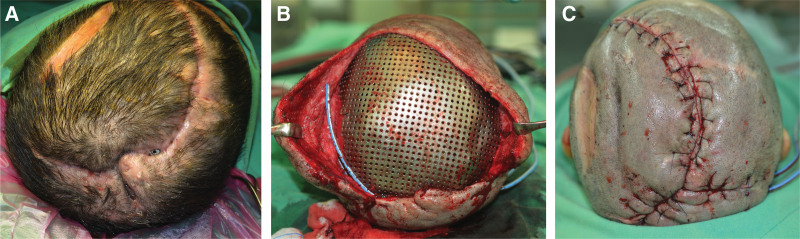
Outcomes: Of all reconstructive procedures for cranioplasty failure, 55.56% was local flap with or without skin graft (n = 10), 16.67% was free flap (n = 3), 11.11% was skin graft only (n = 2), 5.56% was regional flap (n = 1). The free flap survival rate was 100% (3/3), and implant removal with sebsquent second cranioplasty was performed on 27.78% (n = 5) of the patients.
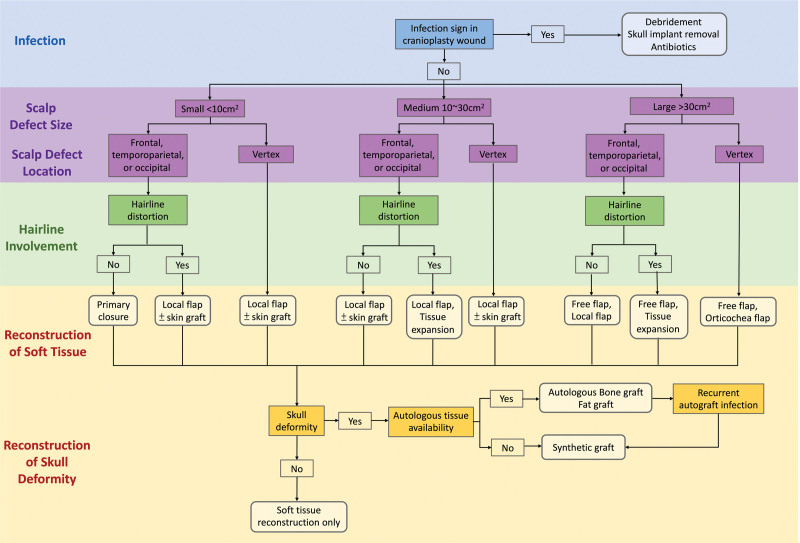
Lessons: Management of cranioplasty failure can be challenging due to infection, refractory implant exposure, and wound dehiscence. The principles of management are based on adequate infection control and reconstructive ladder. Meanwhile, collaboration with plastic surgery and neurosurgery should be strengthened in order to achieve the best clinical outcomes.
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures


References
-
- Alkhaibary A, Alharbi A, Alnefaie N, et al. . Cranioplasty: a comprehensive review of the history, materials, surgical aspects, and complications. World Neurosurg. 2020;139:445–52. - PubMed
-
- Ashayeri K, E MJ, Huang J, et al. . Syndrome of the trephined: a systematic review. Neurosurgery. 2016;79:525–34. - PubMed
-
- Annan M, De Toffol B, Hommet C, et al. . Sinking skin flap syndrome (or Syndrome of the trephined): a review. Br J Neurosurg. 2015;29:314–8. - PubMed
-
- Pertschuk MJ, Whitaker LA. Social and psychological effects of craniofacial deformity and surgical reconstruction. Clin Plast Surg. 1982;9:297–306. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
