

Safety of Sodium-Glucose Cotransporter-2 Inhibitors in Patients with CKD and Type 2 Diabetes: Population-Based US Cohort Study
- PMID: 36827225
- PMCID: PMC10278835
- DOI: 10.2215/CJN.0000000000000115
Safety of Sodium-Glucose Cotransporter-2 Inhibitors in Patients with CKD and Type 2 Diabetes: Population-Based US Cohort Study
Abstract
Background: Limited information exists regarding the safety of sodium-glucose cotransporter-2 inhibitors (SGLT2i) in patients with CKD treated in routine care. We evaluated the safety of SGLT2i in patients with CKD and type 2 diabetes treated in US routine practice.
Methods: Using claims data from Medicare and two large US commercial databases (April 2013-December 2021), we included 96,128 adults with CKD stages 3-4 and type 2 diabetes who newly filled prescriptions for SGLT2i versus glucagon-like peptide-1 receptor agonists (GLP-1RA). Safety outcomes included diabetic ketoacidosis (DKA), lower limb amputations, nonvertebral fractures, genital infections, hypovolemia, AKI, hypoglycemia, and severe urinary tract infections (UTIs). Hazard ratios (HRs) and incidence rate differences per 1000 person-years were estimated after 1:1 propensity score matching, adjusted for >120 baseline characteristics.
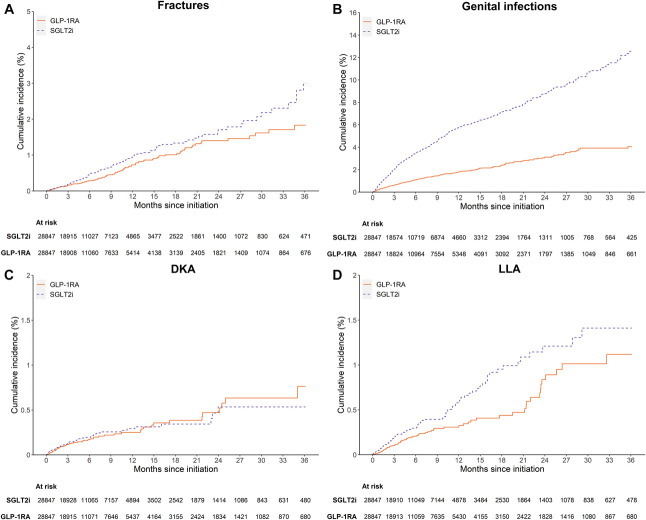
Results: Compared with GLP-1RA, SGLT2i initiators had a higher risk of nonvertebral fractures (HR, 1.30 [95% confidence interval (CI), 1.03 to 1.65]; incidence rate difference, 2.13 [95% CI, 0.28 to 3.97]), lower limb amputations (HR, 1.65 [95% CI, 1.22 to 2.23]; incidence rate difference, 2.46 [95% CI, 1.00 to 3.92]), and genital infections (HR, 3.08 [95% CI, 2.73 to 3.48]; incidence rate difference, 41.26 [95% CI, 37.06 to 45.46]). Similar risks of DKA (HR, 1.07 [95% CI, 0.74 to 1.54]; incidence rate difference, 0.29 [95% CI, -0.89 to 1.46]), hypovolemia (HR, 0.99 [95% CI, 0.86 to 1.14]; incidence rate difference, 0.20 [95% CI, -2.85 to 3.25]), hypoglycemia (HR, 1.08 [95% CI, 0.92 to 1.26]; incidence rate difference, 1.46 [95% CI, -1.31 to 4.23]), and severe UTI (HR, 1.02 [95% CI, 0.87 to 1.19]; incidence rate difference, 0.35 [95% CI, -2.51 to 3.21]) were observed. SGLT2i had lower risk for AKI (HR, 0.93 [95% CI, 0.87 to 0.99]; incidence rate difference, -6.75 [95% CI, -13.69 to 0.20]).
Conclusions: In US patients with CKD and type 2 diabetes receiving routine care, SGLT2i use was associated with higher risks of genital infections and potentially lower limb amputations and nonvertebral fractures.
Copyright © 2023 by the American Society of Nephrology.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
