

Predicting Outcomes of Language Rehabilitation: Prognostic Factors for Immediate and Long-Term Outcomes After Aphasia Therapy
- PMID: 36827514
- PMCID: PMC10205105
- DOI: 10.1044/2022_JSLHR-22-00347
Predicting Outcomes of Language Rehabilitation: Prognostic Factors for Immediate and Long-Term Outcomes After Aphasia Therapy
Abstract
Background: Aphasia therapy is an effective approach to improve language function in chronic aphasia. However, it remains unclear what prognostic factors facilitate therapy response at the individual level. Here, we utilized data from the POLAR (Predicting Outcomes of Language Rehabilitation in Aphasia) trial to (a) determine therapy-induced change in confrontation naming and long-term maintenance of naming gains and (b) examine the extent to which aphasia severity, age, education, time postonset, and cognitive reserve predict naming gains at 1 week, 1 month, and 6 months posttherapy.
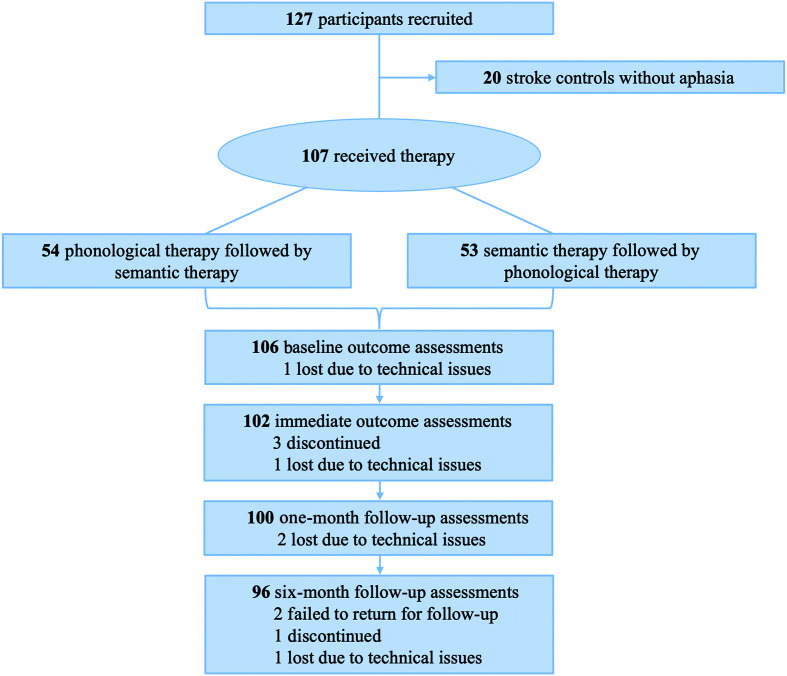
Method: A total of 107 participants with chronic (≥ 12 months poststroke) aphasia underwent extensive case history, cognitive-linguistic testing, and a neuroimaging workup prior to receiving 6 weeks of impairment-based language therapy. Therapy-induced change in naming performance (measured as raw change on the 175-item Philadelphia Naming Test [PNT]) was assessed 1 week after therapy and at follow-up time points 1 month and 6 months after therapy completion. Change in naming performance over time was evaluated using paired t tests, and linear mixed-effects models were constructed to examine the association between prognostic factors and therapy outcomes.
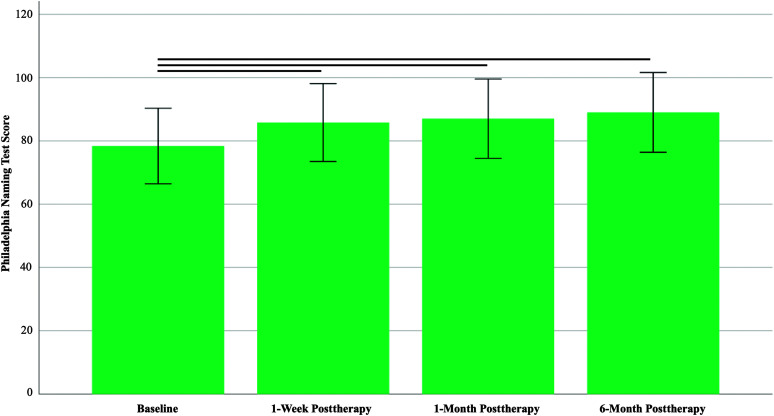
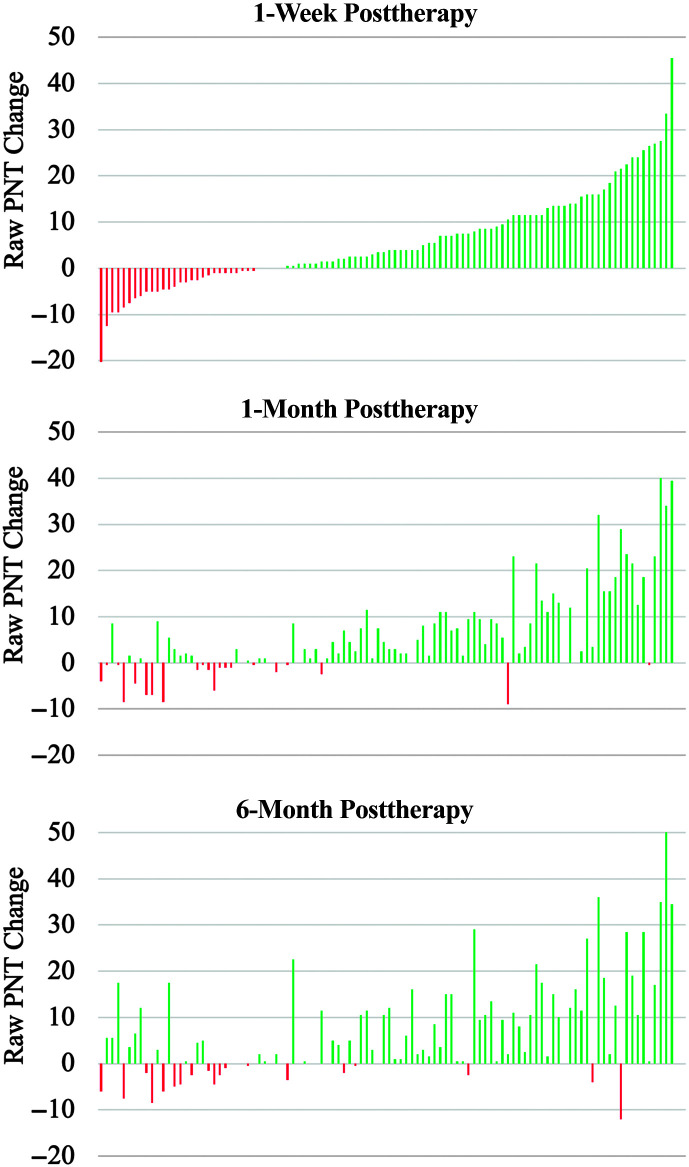
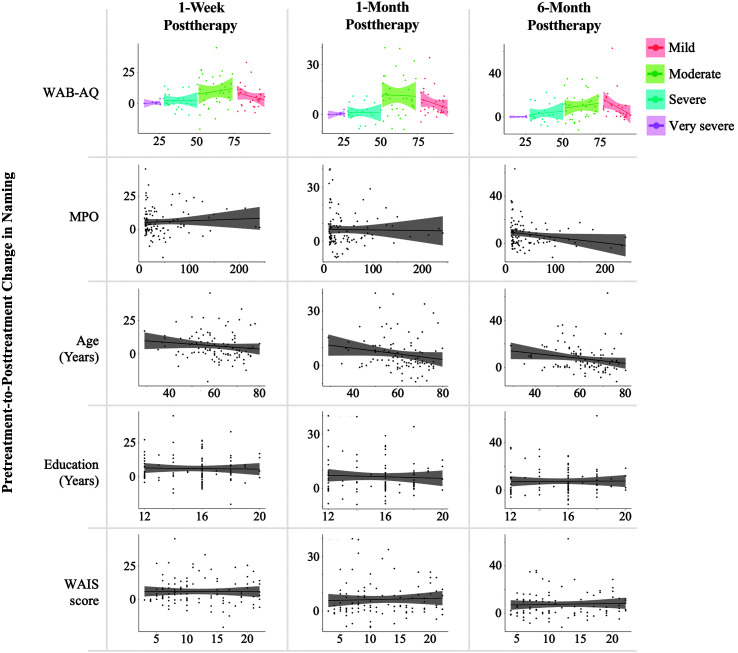
Results: Naming performance was improved by 5.9 PNT items (Cohen's d = 0.56, p < .001) 1 week after therapy and by 6.4 (d = 0.66, p < .001) and 7.5 (d = 0.65, p < .001) PNT items at 1 month and 6 months after therapy completion, respectively. Aphasia severity emerged as the strongest predictor of naming improvement recovery across time points; mild (ß = 5.85-9.02) and moderate (ß = 9.65-11.54) impairment predicted better recovery than severe (ß = 1.31-3.37) and very severe (ß = 0.20-0.32) aphasia. Age was an emergent prognostic factor for recovery 1 month (ß = -0.14) and 6 months (ß = -0.20) after therapy, and time postonset (ß = -0.05) was associated with retention of naming gains at 6 months posttherapy.
Conclusions: These results suggest that therapy-induced naming improvement is predictable based on several easily measurable prognostic factors. Broadly speaking, these results suggest that prognostication procedures in aphasia therapy can be improved and indicate that personalization of therapy is a realistic goal in the near future.
Supplemental material: https://doi.org/10.23641/asha.22141829.
Figures


References
-
- Adamson, J. , Beswick, A. , & Ebrahim, S. (2004). Is stroke the most common cause of disability? Journal of Stroke & Cerebrovascular Diseases, 13(4), 171–177. https://doi.org/10.1016/j.jstrokecerebrovasdis.2004.06.003 - PubMed
-
- Alexander, D. L. J. , Tropsha, A. , & Winkler, D. A. (2015). Beware of R 2: Simple, unambiguous assessment of the prediction accuracy of QSAR and QSPR models. Journal of Chemical Information and Modeling, 55(7), 1316–1322. https://doi.org/10.1021/acs.jcim.5b00206 - PMC - PubMed
-
- Ali, M. , Lyden, P. , Brady, M. , & VISTA Collaboration. (2015). Aphasia and dysarthria in acute stroke: Recovery and functional outcome. International Journal of Stroke, 10(3), 400–406. https://doi.org/10.1111/ijs.12067 - PubMed
-
- Basso, A. (1992). Prognostic factors in aphasia. Aphasiology, 6(4), 337–348. https://doi.org/10.1080/02687039208248605
-
- Berube, S. , & Hillis, A. E. (2019). Advances and innovations in aphasia treatment trials. Stroke, 50(10), 2977–2984. https://doi.org/10.1161/STROKEAHA.119.025290 - PMC - PubMed
