

Pros and Cons of Dual-Energy CT Systems: "One Does Not Fit All"
- PMID: 36828369
- PMCID: PMC9964233
- DOI: 10.3390/tomography9010017
Pros and Cons of Dual-Energy CT Systems: "One Does Not Fit All"
Abstract
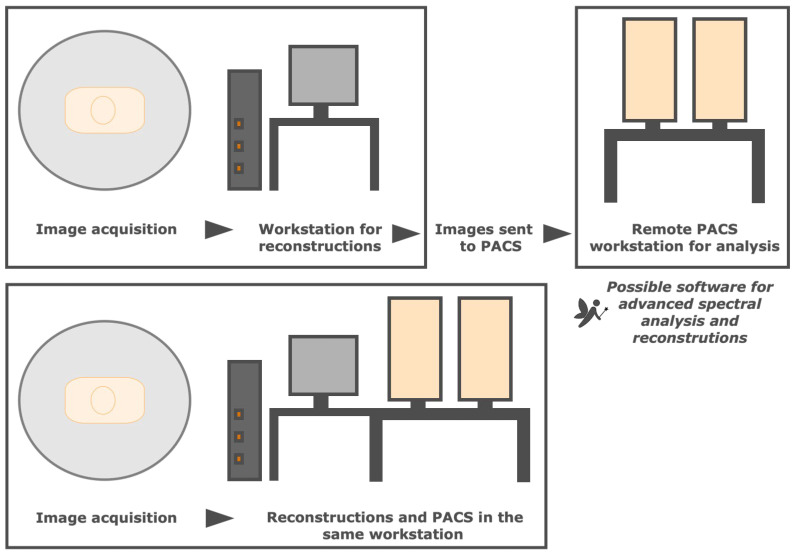
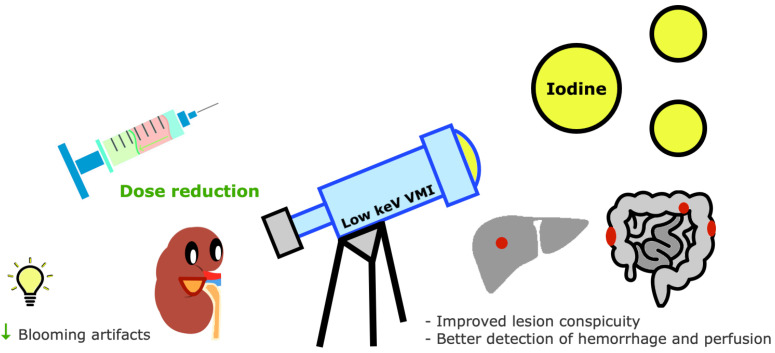
Dual-energy computed tomography (DECT) uses different energy spectrum x-ray beams for differentiating materials with similar attenuation at a certain energy. Compared with single-energy CT, it provides images with better diagnostic performance and a potential reduction of contrast agent and radiation doses. There are different commercially available DECT technologies, with machines that may display two x-ray sources and two detectors, a single source capable of fast switching between two energy levels, a specialized detector capable of acquiring high- and low-energy data sets, and a filter splitting the beam into high- and low-energy beams at the output. Sequential acquisition at different tube voltages is an alternative approach. This narrative review describes the DECT technique using a Q&A format and visual representations. Physical concepts, parameters influencing image quality, postprocessing methods, applicability in daily routine workflow, and radiation considerations are discussed. Differences between scanners are described, regarding design, image quality variabilities, and their advantages and limitations. Additionally, current clinical applications are listed, and future perspectives for spectral CT imaging are addressed. Acknowledging the strengths and weaknesses of different DECT scanners is important, as these could be adapted to each patient, clinical scenario, and financial capability. This technology is undoubtedly valuable and will certainly keep improving.
Keywords: dual-energy CT; dual-layer detector CT; dual-source CT; fast kVp switching; image quality; photon counting; spectral CT; split-filter.
Conflict of interest statement
The authors declare no conflict of interest.
Figures












References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
