

Comparison of COVID-19 hospitalization costs across care pathways: a patient-level time-driven activity-based costing analysis in a Brazilian hospital
- PMID: 36829122
- PMCID: PMC9955521
- DOI: 10.1186/s12913-023-09049-8
Comparison of COVID-19 hospitalization costs across care pathways: a patient-level time-driven activity-based costing analysis in a Brazilian hospital
Abstract
Background: The COVID-19 pandemic raised awareness of the need to better understand where and how patient-level costs are incurred in health care organizations, as health managers and other decision-makers need to plan and quickly adapt to the increasing demand for health care services to meet patients' care needs. Time-driven activity-based costing offers a better understanding of the drivers of cost throughout the care pathway, providing information that can guide decisions on process improvement and resource optimization. This study aims to estimate COVID-19 patient-level hospital costs and to evaluate cost variability considering the in-hospital care pathways of COVID-19 management and the patient clinical classification.
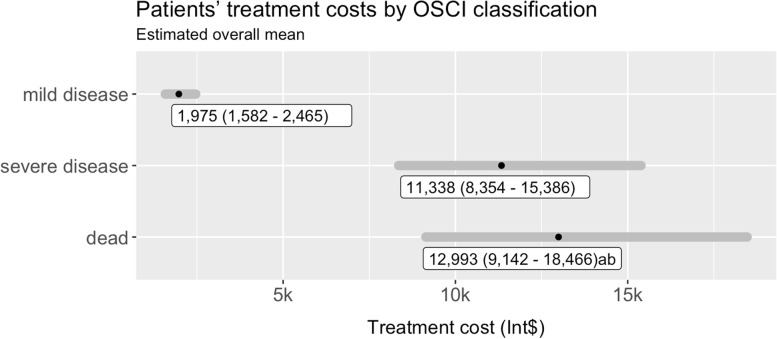
Methods: This is a prospective cohort study that applied time-driven activity-based costing (TDABC) in a Brazilian reference center for COVID-19. Patients hospitalized during the first wave of the disease were selected for their data to be analyzed to estimate in-hospital costs. The cost information was calculated at the patient level and stratified by hospital care pathway and Ordinal Scale for Clinical Improvement (OSCI) category. Multivariable analyses were applied to identify predictors of cost variability in the care pathways that were evaluated.
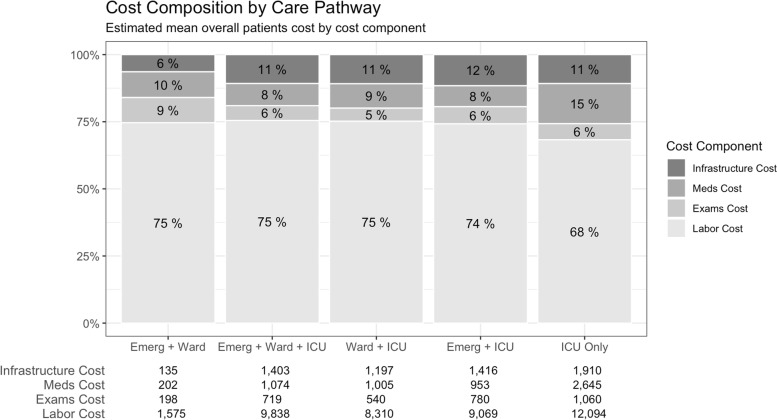
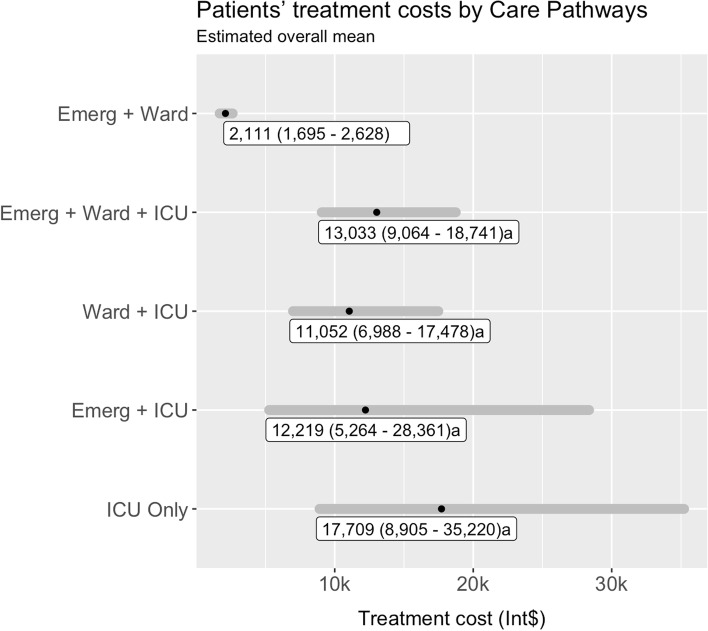
Results: A total of 208 patients were included in the study. Patients followed five different care pathways, of which Emergency + Ward was the most followed (n = 118, 57%). Pathways which included the intensive care unit presented a statistically significant influence on costs per patient (p < 0.001) when compared to Emergency + Ward. The median cost per patient was I$2879 (IQR 1215; 8140) and mean cost per patient was I$6818 (SD 9043). The most expensive care pathway was the ICU only, registering a median cost per patient of I$13,519 (IQR 5637; 23,373) and mean cost per patient of I$17,709 (SD 16,020). All care pathways that included the ICU unit registered a higher cost per patient.
Conclusions: This is one of the first microcosting study for COVID-19 that applied the TDABC methodology and demonstrated how patient-level costs vary as a function of the care pathways followed by patients. These findings can be used to develop value reimbursement strategies that will inform sustainable health policies in middle-income countries such as Brazil.
Keywords: COVID-19; Cost and cost analysis; Health care costs; Microcosting; TDABC; Time-driven activity-based costing.
© 2023. The Author(s).
Conflict of interest statement
None reported.
Figures
References
-
- Etges APBS, Bertoglio Cardoso R, Marcolino MS, Brasil Ruschel K, Coutinho AP, Pereira EC, Anschau F, Aranha F, Carrilho F, Vietta G, et al. The economic impact of COVID-19 treatment at a hospital-level: investment and financial registers of Brazilian hospitals. J Health Econ Outcomes Res. 2021;8(1):36–41. doi: 10.36469/jheor.2021.22066. - DOI - PMC - PubMed
-
- Kaplan R, Witkowski M, Abbott M, Guzman A, Higgins L, Meara J, Padden E, Shah A, Waters P, Weidemeier M, et al. Using time-driven activity-based costing to identify value improvement opportunities in healthcare. J Healthcare Manag Am Coll Healthcare Executives. 2014;59:399–412. - PubMed
-
- Allin O, Urman RD, Edwards AF, Blitz JD, Pfeifer KJ, Feeley TW, Bader AM. Using time-driven activity-based costing to demonstrate value in perioperative care: recommendations and review from the Society for Perioperative Assessment and Quality Improvement (SPAQI) J Med Syst. 2019;44(1):25. doi: 10.1007/s10916-019-1503-2. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
