

A novel preoperative inflammation score system established for postoperative prognosis predicting of intrahepatic cholangiocarcinoma
- PMID: 36829168
- PMCID: PMC9951514
- DOI: 10.1186/s12885-023-10668-x
A novel preoperative inflammation score system established for postoperative prognosis predicting of intrahepatic cholangiocarcinoma
Abstract
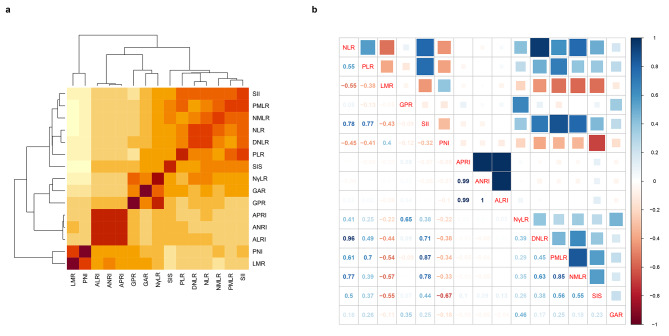
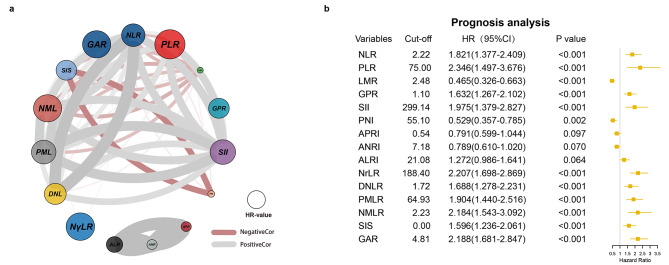
Background: Inflammation is implicated in tumorigenesis and has been reported as an important prognostic factor in cancers. In this study, we aimed to develop and validate a novel inflammation score (IFS) system based on 12 inflammatory markers and explore its impact on intrahepatic cholangiocarcinoma (ICC) survival after hepatectomy.
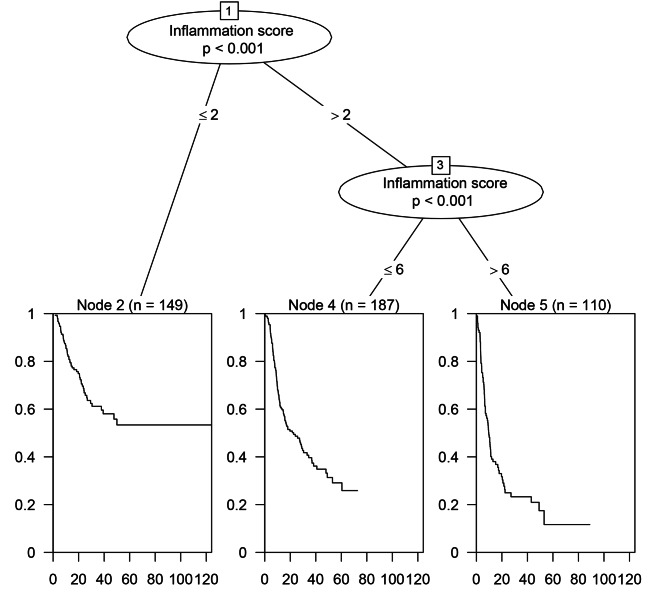
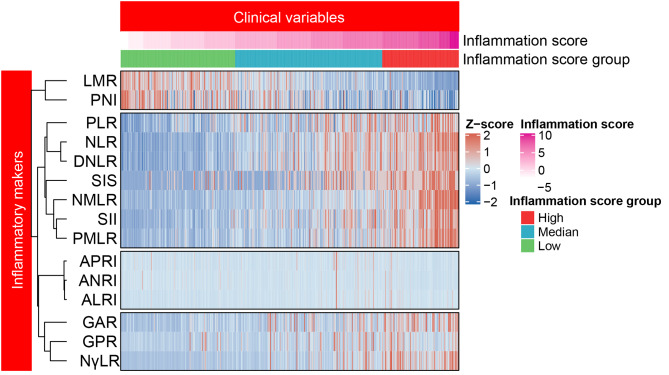
Methods: Clinical data of 446 ICC patients undergoing surgical treatment were collected from the Primary Liver Cancer Big Data, and then served as a training cohort to establish the IFS. Furthermore, an internal validation cohort including 175 patients was used as internal validation cohort of the IFS. A survival tree analysis was used to divide ICC patients into three groups (low-, median-, and high- IFS-score groups) according to different IFS values. Kaplan-Meier (KM) curves were used to compare the overall survival (OS) and recurrence-free survival (RFS) rates among three different groups. Cox regression analyses were applied to explore the independent risk factors influencing OS and RFS.
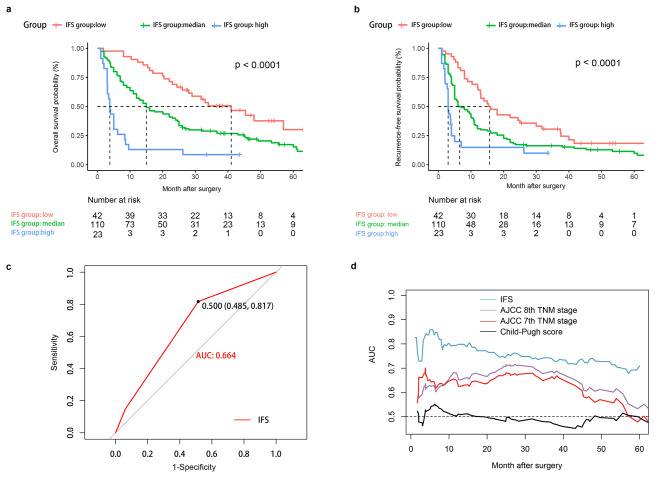
Results: In the training cohort, 149 patients were in the low-IFS-score group, 187 in the median-IFS-score group, and 110 in the high-IFS-score group. KM curves showed that the high-IFS-score group had worse OS and RFS rates than those of the low- and median-IFS-score groups (P < 0.001) in both the training and validation cohorts. Moreover, multivariable Cox analyses identified high IFS as an independent risk factor for OS and RFS in the training cohort. The area under the curve values for OS prediction of IFS were 0.703 and 0.664 in the training and validation cohorts, respectively, which were higher than those of the American Joint Committee on Cancer (AJCC) 7th edition TNM stage, AJCC 8th edition TNM stage, and the Child-Pugh score.
Conclusion: Our results revealed the IFS was an independent risk factor for OS and RFS in patients with ICC after hepatectomy and could serve as an effective prognostic prediction system in daily clinical practice.
Keywords: Intrahepatic cholangiocarcinoma; Liver resection; Prognosis; Systemic inflammation.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
Development and validation of a new prognostic immune-inflammatory-nutritional score for predicting outcomes after curative resection for intrahepatic cholangiocarcinoma: A multicenter study.Front Immunol. 2023 Mar 31;14:1165510. doi: 10.3389/fimmu.2023.1165510. eCollection 2023. Front Immunol. 2023. PMID: 37063918 Free PMC article.
-
The prognostic value of sarcopenia combined with hepatolithiasis in intrahepatic cholangiocarcinoma patients after surgery: A prospective cohort study.Eur J Surg Oncol. 2021 Mar;47(3 Pt B):603-612. doi: 10.1016/j.ejso.2020.09.002. Epub 2020 Sep 6. Eur J Surg Oncol. 2021. PMID: 32933804
-
[The prognostic value of preoperative peripheral blood inflammatory biomarkers for intrahepatic cholangiocarcinoma after radical resection].Zhonghua Zhong Liu Za Zhi. 2022 Nov 23;44(11):1194-1201. doi: 10.3760/cma.j.cn112152-20210324-00265. Zhonghua Zhong Liu Za Zhi. 2022. PMID: 36380668 Chinese.
-
Prognostic analysis of patients with combined hepatocellular-cholangiocarcinoma after radical resection: A retrospective multicenter cohort study.World J Gastroenterol. 2022 Nov 7;28(41):5968-5981. doi: 10.3748/wjg.v28.i41.5968. World J Gastroenterol. 2022. PMID: 36405111 Free PMC article. Review.
-
Predictors of Distant Metastasis and Prognosis in Newly Diagnosed T1 Intrahepatic Cholangiocarcinoma.Biomed Res Int. 2023 Jan 17;2023:6638755. doi: 10.1155/2023/6638755. eCollection 2023. Biomed Res Int. 2023. PMID: 36704724 Free PMC article. Review.
Cited by
-
Lymphocyte-to-Monocyte Ratio and Clinical Outcomes in Cholangiocarcinoma: A Systematic Review and Meta-Analysis.Diagnostics (Basel). 2022 Nov 1;12(11):2655. doi: 10.3390/diagnostics12112655. Diagnostics (Basel). 2022. PMID: 36359498 Free PMC article. Review.
-
Malignant cell receptor-ligand subtypes guide the prediction of prognosis and personalized immunotherapy of liver cancer.Aging (Albany NY). 2024 Jan 18;16(2):1712-1732. doi: 10.18632/aging.205453. Epub 2024 Jan 18. Aging (Albany NY). 2024. PMID: 38244584 Free PMC article.
-
Prognostic value of the Naples prognostic score in patients with intrahepatic cholangiocarcinoma after hepatectomy.BMC Cancer. 2024 Jun 14;24(1):727. doi: 10.1186/s12885-024-12502-4. BMC Cancer. 2024. PMID: 38877445 Free PMC article.
-
Unveiling the prognostic role of blood inflammatory indexes in a retrospective cohort of patients undergoing liver resection for intrahepatic cholangiocarcinoma.Int J Surg. 2024 Nov 1;110(11):7088-7096. doi: 10.1097/JS9.0000000000001924. Int J Surg. 2024. PMID: 38967502 Free PMC article.
-
Epidemiology of biliary tract cancer in China: A narrative review.Chin J Cancer Res. 2024 Oct 30;36(5):474-488. doi: 10.21147/j.issn.1000-9604.2024.05.02. Chin J Cancer Res. 2024. PMID: 39539810 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
