

Carotid body paraganglioma metastatic to spine causing cord compression: a case report
- PMID: 36829189
- PMCID: PMC9951469
- DOI: 10.1186/s13000-023-01314-y
Carotid body paraganglioma metastatic to spine causing cord compression: a case report
Abstract
Background: Carotid body tumors (CBTs) are rare neuroendocrine neoplasms arising near the carotid bifurcation with a reported incidence of 1 to 2 cases in 100,000 patients. Most CBTs are sporadic, benign, slow-growing, and non-secreting, but untreated CBTs can grow locally to compress the nearby blood vessels, esophagus, and airway. Regional metastases can occur in 5% to 10% of cases, but distant metastases are exceedingly rare, occurring in roughly 1-2% of cases. As such, the optimal treatment for metastatic CBTs is not well-defined. We report a rare case of a patient with CBT distant metastases causing spinal cord compression.
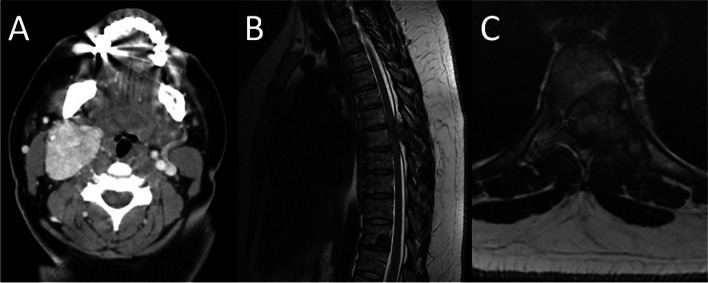
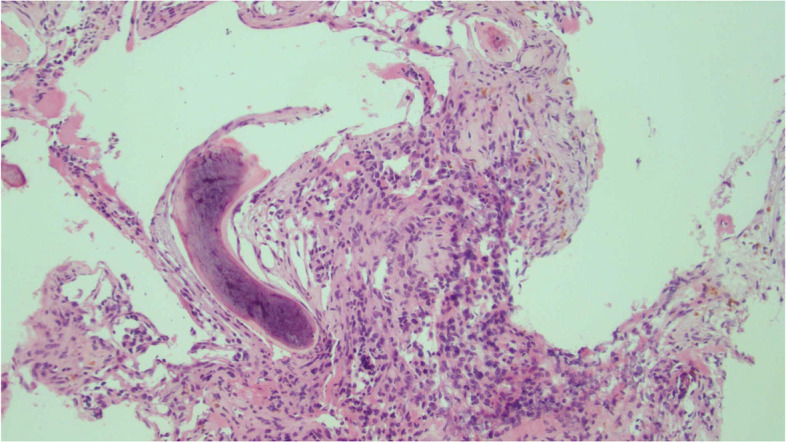
Case presentation: A 40-year-old African American female presented with a right neck mass, headaches, vertigo, tinnitus, hoarseness, and dysphagia. Imaging demonstrated a Shamblin II right neck mass; subsequent transcervical resection and pathology showed a carotid body paraganglioma. The patient recurred locally near the carotid bifurcation, so she underwent Stereotactic Body Radiation Therapy to the recurrent right neck disease. She later re-presented with new onset bilateral lower extremity weakness, dysmetria, and numbness. She was found to have metastatic disease to the thoracic spine causing spinal cord compression. She underwent laminectomy, tumor resection, and posterior fixation followed by adjuvant radiation therapy. She was started on systemic therapy with sunitinib. She eventually progressed with metastatic disease to the right iliac bone, which was treated with palliative radiotherapy. Second line systemic therapy with capecitabine and temozolomide was started. At last follow up, the patient was asymptomatic with stable persistent disease.
Conclusions: Paragangliomas often exhibit a prolonged interval to the development of progression; locoregional recurrences or rare distant metastases have been reported to occur as many as 20 years from diagnosis. The natural course of CBTs in other cases as well as the present case call into question the idea that CBTs are truly benign; instead CBTs may be indolent tumors with metastatic potential. Treatment choices for CBTs include surgical resection, radiation therapy, and systemic therapy, though the optimal treatment regimen for metastatic CBTs is not well-defined. A more advanced understanding of CBT pathophysiology, disease classification, risk stratification, and treatment options is needed to improve outcomes for patients.
Keywords: Carotid body tumor; Cord compression; Metastatic; Paraganglioma; Radiotherapy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Treatment of metastatic carotid body paraganglioma in a young female.J Surg Case Rep. 2024 Dec 26;2025(1):rjae811. doi: 10.1093/jscr/rjae811. eCollection 2025 Jan. J Surg Case Rep. 2024. PMID: 39726575 Free PMC article.
-
Carotid Body Tumor Microenvironment.Adv Exp Med Biol. 2020;1296:151-162. doi: 10.1007/978-3-030-59038-3_9. Adv Exp Med Biol. 2020. PMID: 34185291
-
Malignant carotid body tumor: a report of two cases.Ann Med Surg (Lond). 2023 Apr 11;85(5):1857-1862. doi: 10.1097/MS9.0000000000000402. eCollection 2023 May. Ann Med Surg (Lond). 2023. PMID: 37229046 Free PMC article.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Multiple spinal metastases from paraganglioma.Cancer. 1990 Nov 15;66(10):2224-8. doi: 10.1002/1097-0142(19901115)66:10<2224::aid-cncr2820661031>3.0.co;2-e. Cancer. 1990. PMID: 2224778 Review.
References
-
- SevillaGarcía MA, LlorentePendás JL, Rodrigo Tapia JP, et al. Head and neck paragangliomas: revision of 89 cases in 73 patients. Acta Otorrinolaringol Esp. 2007;58(3):94–100. - PubMed
-
- Naylor R. Extracranial carotid and vertebral artery disease. In: Aboyans V, ed. ESC CardioMed. Oxford University Press; 2018:2704–2712. 10.1093/med/9780198784906.003.0778.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
