

Targeted plasma proteomics reveals signatures discriminating COVID-19 from sepsis with pneumonia
- PMID: 36829233
- PMCID: PMC9950694
- DOI: 10.1186/s12931-023-02364-y
Targeted plasma proteomics reveals signatures discriminating COVID-19 from sepsis with pneumonia
Abstract
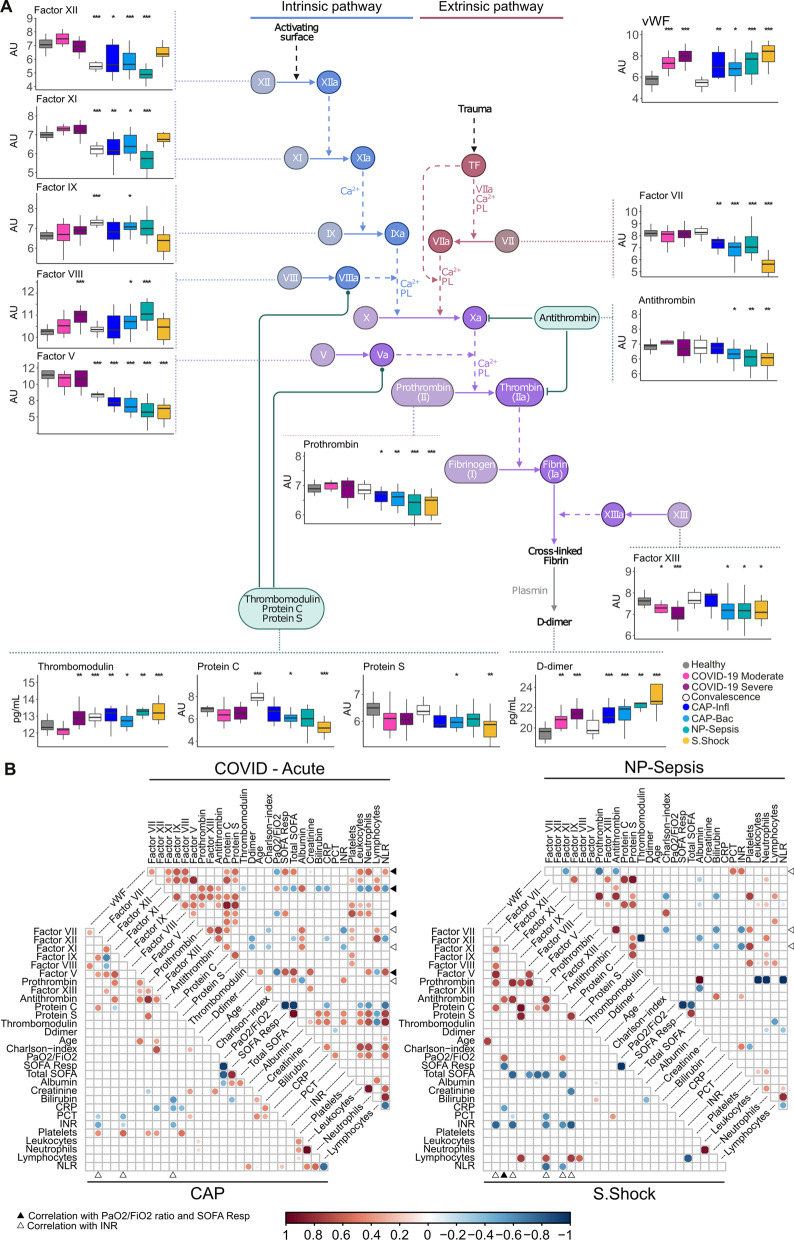
Background: COVID-19 remains a major public health challenge, requiring the development of tools to improve diagnosis and inform therapeutic decisions. As dysregulated inflammation and coagulation responses have been implicated in the pathophysiology of COVID-19 and sepsis, we studied their plasma proteome profiles to delineate similarities from specific features.
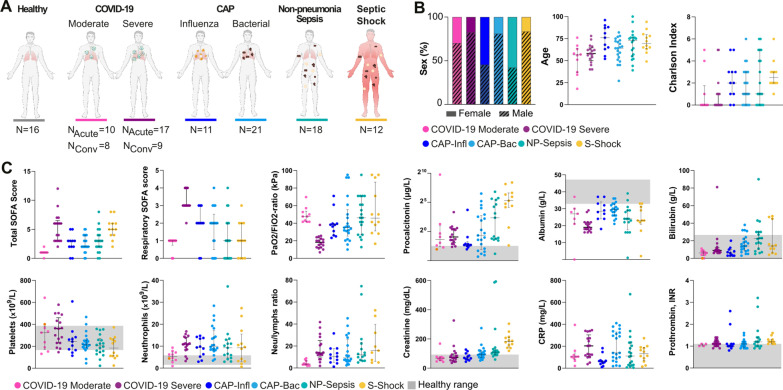
Methods: We measured 276 plasma proteins involved in Inflammation, organ damage, immune response and coagulation in healthy controls, COVID-19 patients during acute and convalescence phase, and sepsis patients; the latter included (i) community-acquired pneumonia (CAP) caused by Influenza, (ii) bacterial CAP, (iii) non-pneumonia sepsis, and (iv) septic shock patients.
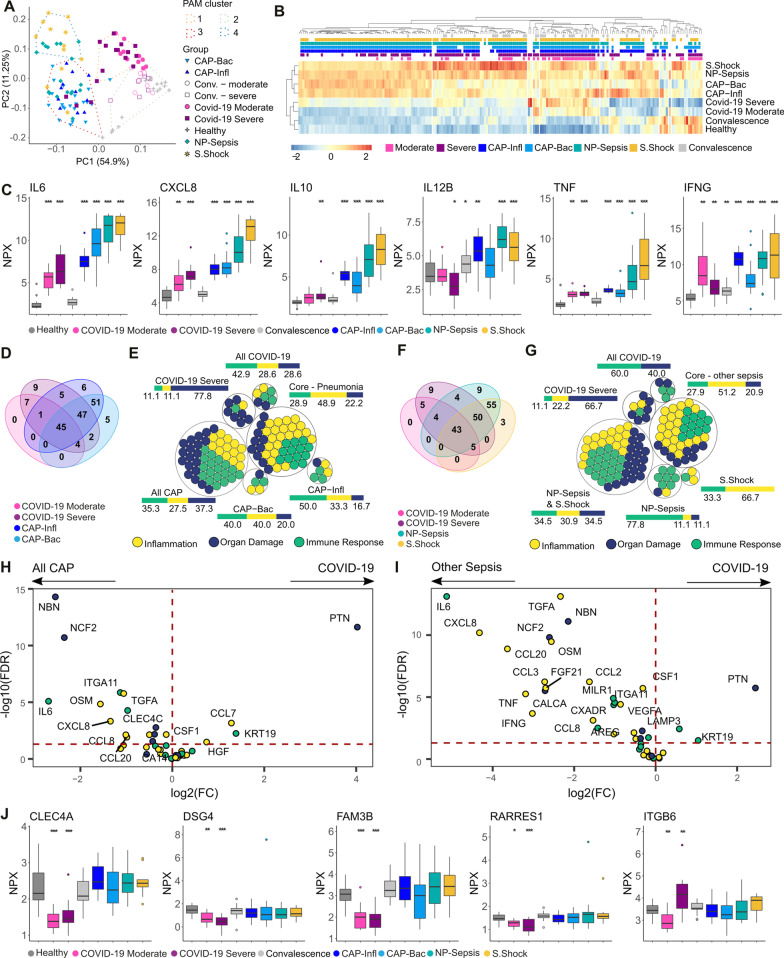
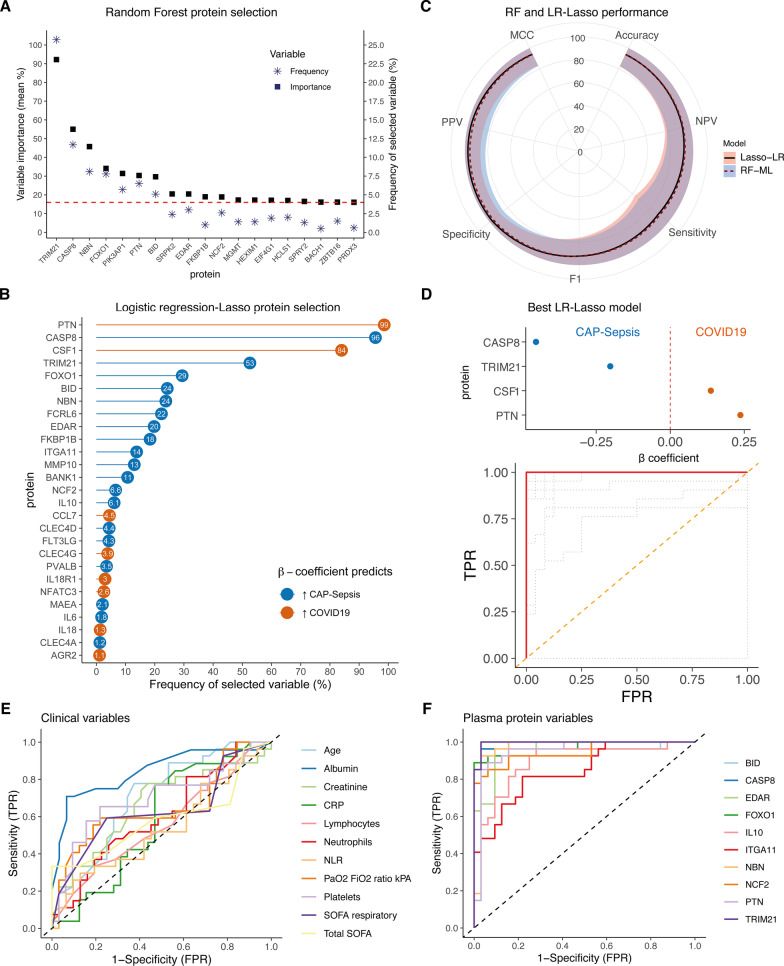
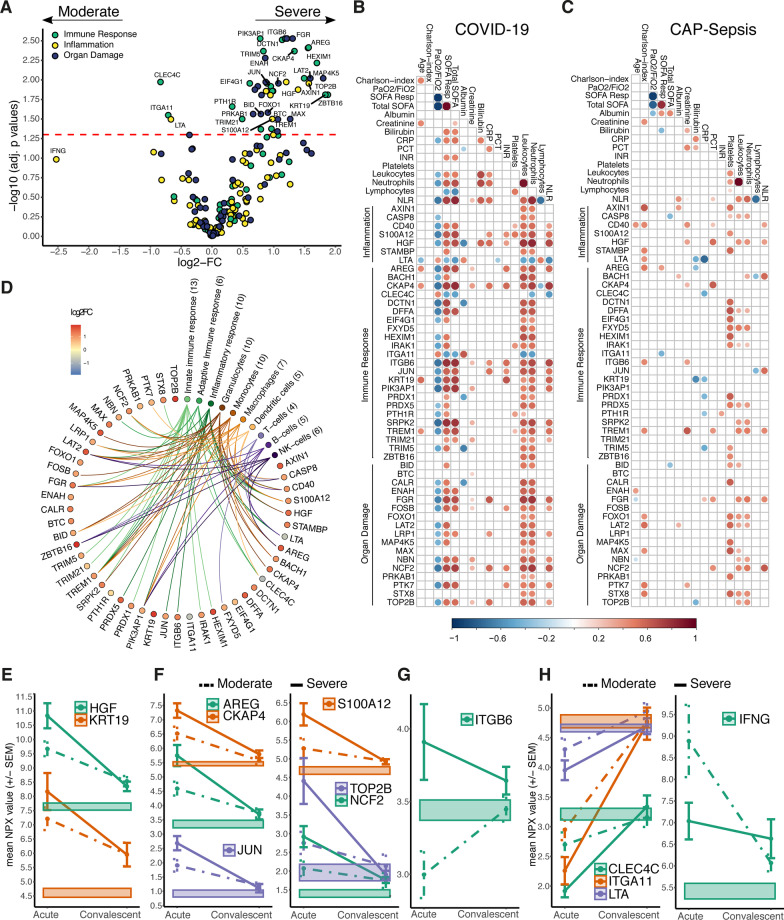
Results: We identified a core response to infection consisting of 42 proteins altered in both COVID-19 and sepsis, although higher levels of cytokine storm-associated proteins were evident in sepsis. Furthermore, microbiologic etiology and clinical endotypes were linked to unique signatures. Finally, through machine learning, we identified biomarkers, such as TRIM21, PTN and CASP8, that accurately differentiated COVID-19 from CAP-sepsis with higher accuracy than standard clinical markers.
Conclusions: This study extends the understanding of host responses underlying sepsis and COVID-19, indicating varying disease mechanisms with unique signatures. These diagnostic and severity signatures are candidates for the development of personalized management of COVID-19 and sepsis.
Keywords: COVID-19; Community acquired pneumonia; Olink proximity extension assays; Sepsis; Septic shock.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
