

Comparing 3D, 2.5D, and 2D Approaches to Brain Image Auto-Segmentation
- PMID: 36829675
- PMCID: PMC9952534
- DOI: 10.3390/bioengineering10020181
Comparing 3D, 2.5D, and 2D Approaches to Brain Image Auto-Segmentation
Abstract
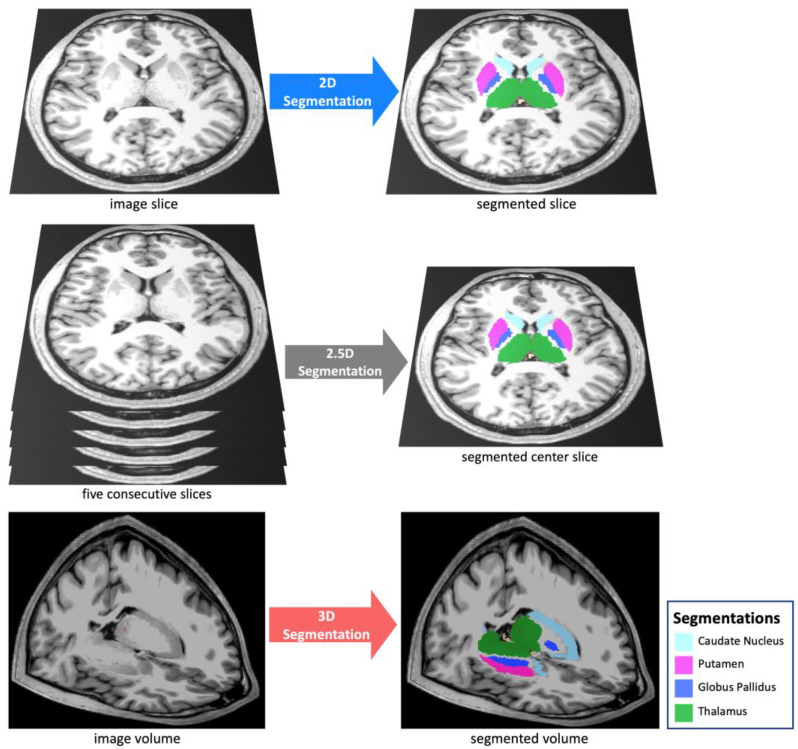
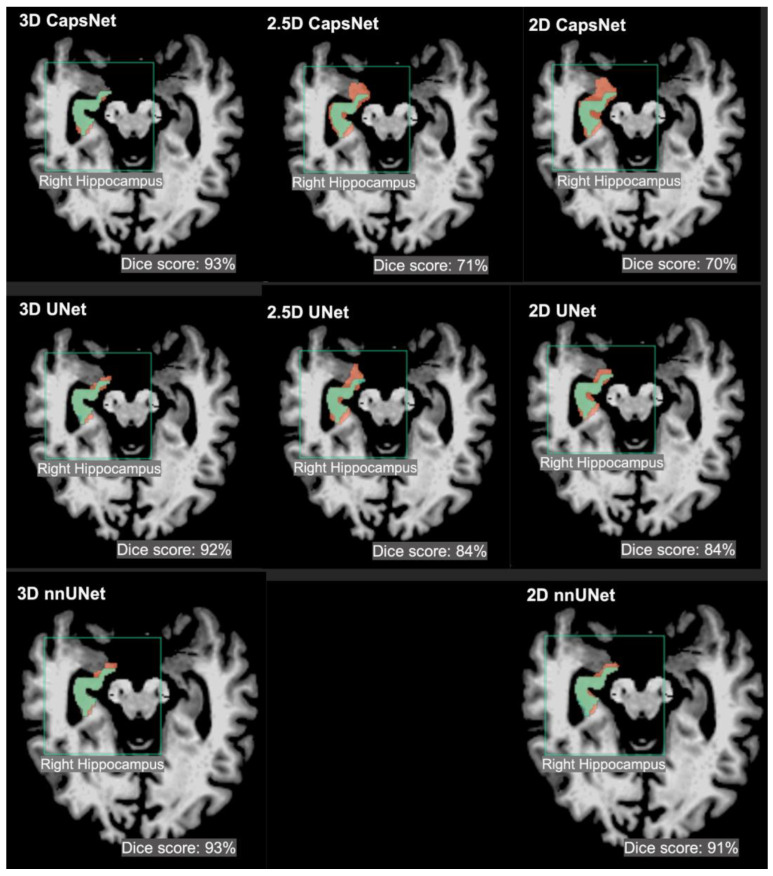
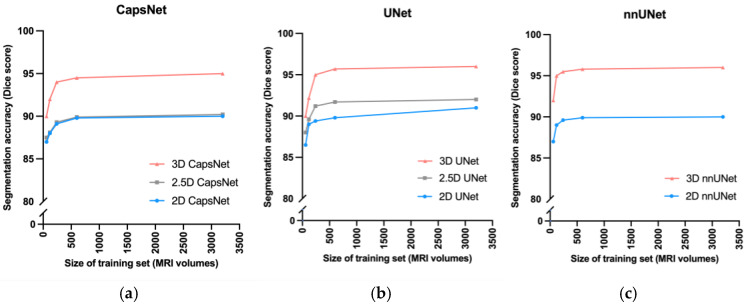
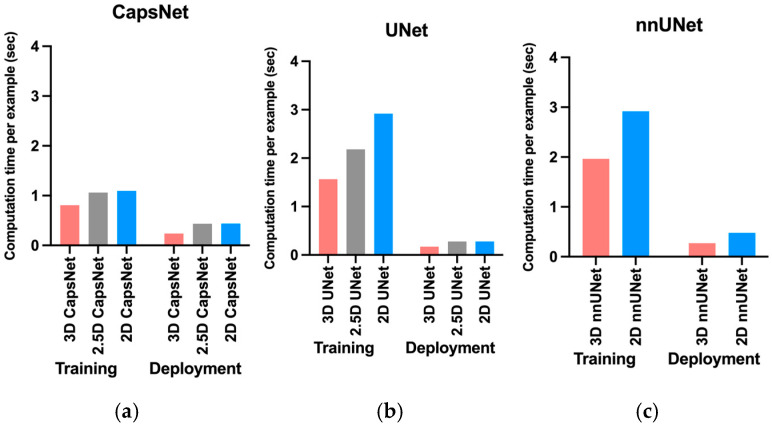
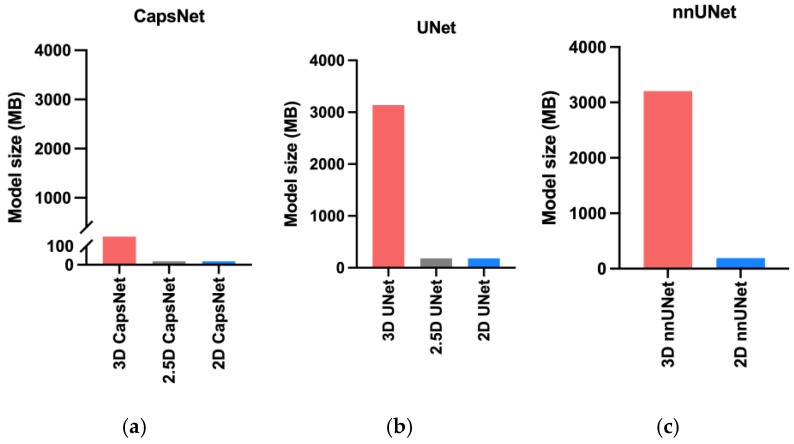
Deep-learning methods for auto-segmenting brain images either segment one slice of the image (2D), five consecutive slices of the image (2.5D), or an entire volume of the image (3D). Whether one approach is superior for auto-segmenting brain images is not known. We compared these three approaches (3D, 2.5D, and 2D) across three auto-segmentation models (capsule networks, UNets, and nnUNets) to segment brain structures. We used 3430 brain MRIs, acquired in a multi-institutional study, to train and test our models. We used the following performance metrics: segmentation accuracy, performance with limited training data, required computational memory, and computational speed during training and deployment. The 3D, 2.5D, and 2D approaches respectively gave the highest to lowest Dice scores across all models. 3D models maintained higher Dice scores when the training set size was decreased from 3199 MRIs down to 60 MRIs. 3D models converged 20% to 40% faster during training and were 30% to 50% faster during deployment. However, 3D models require 20 times more computational memory compared to 2.5D or 2D models. This study showed that 3D models are more accurate, maintain better performance with limited training data, and are faster to train and deploy. However, 3D models require more computational memory compared to 2.5D or 2D models.
Keywords: auto-segmentation; deep learning; magnetic resonance imaging; neuroimaging.
Conflict of interest statement
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Dasenbrock H.H., See A.P., Smalley R.J., Bi W.L., Dolati P., Frerichs K.U., Golby A.J., Chiocca E.A., Aziz-Sultan M.A. Frameless Stereotactic Navigation during Insular Glioma Resection using Fusion of Three-Dimensional Rotational Angiography and Magnetic Resonance Imaging. World Neurosurg. 2019;126:322–330. doi: 10.1016/j.wneu.2019.03.096. - DOI - PubMed
-
- Bousabarah K., Ruge M., Brand J.-S., Hoevels M., Rueß D., Borggrefe J., Hokamp N.G., Visser-Vandewalle V., Maintz D., Treuer H., et al. Deep convolutional neural networks for automated segmentation of brain metastases trained on clinical data. Radiat. Oncol. 2020;15:87. doi: 10.1186/s13014-020-01514-6. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
