

Cardiac Resynchronization Therapy and Hypertrophic Cardiomyopathy: A Comprehensive Review
- PMID: 36830887
- PMCID: PMC9952999
- DOI: 10.3390/biomedicines11020350
Cardiac Resynchronization Therapy and Hypertrophic Cardiomyopathy: A Comprehensive Review
Abstract
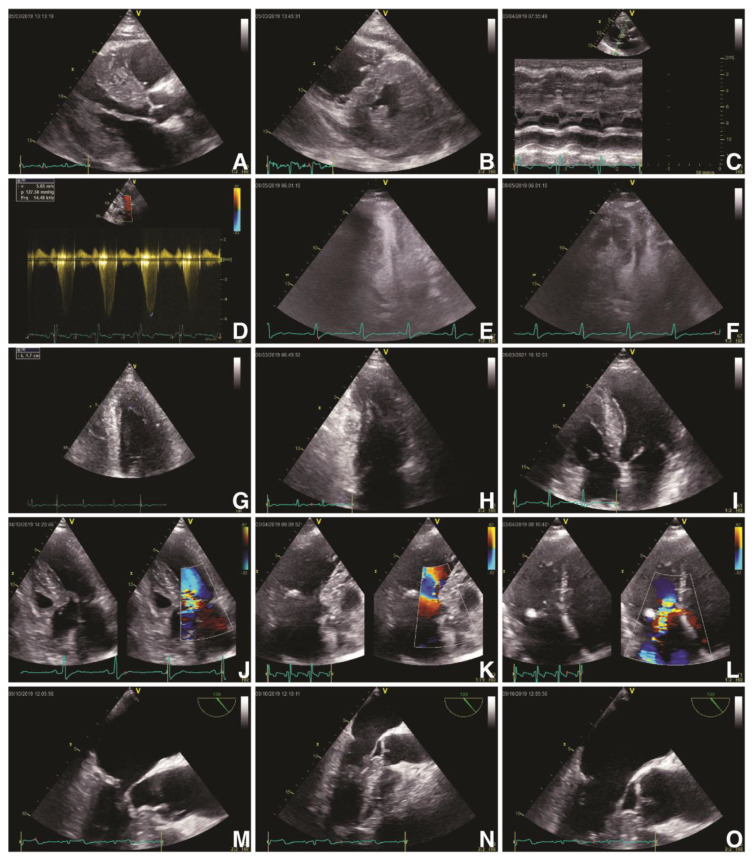
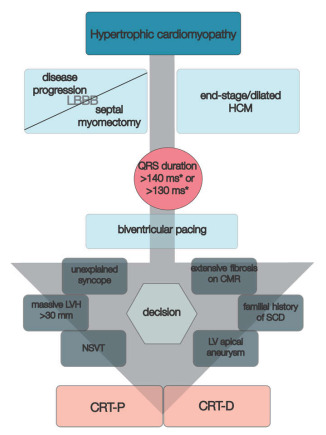
Hypertrophic cardiomyopathy (HCM) is an inherited primary myocardial disease characterized by asymmetrical/symmetrical left ventricle (LV) hypertrophy, with or without LV outflow tract (LVOT) dynamic obstruction, and poor prognosis. Cardiac resynchronization therapy (CRT) has emerged as a minimally invasive tool for patients with heart failure (HF) with decreased LV ejection fraction (LVEF) and prolonged QRS duration of over 120 ms with or without left bundle branch block (LBBB). Several HCM patients are at risk of developing LBBB because of disease progression or secondary to septal myomectomy, while others might develop HF with decreased LVEF, alleged end-stage/dilated HCM, especially those with thin myofilament mutations. Several studies have shown that patients with myectomy-induced LBBB might benefit from left bundle branch pacing or CRT to relieve symptoms, improve exercise capacity, and increase LVEF. Otherwise, patients with end-stage/dilated HCM and prolonged QRS interval could gain from CRT in terms of NYHA class improvement, LV systolic performance increase and, to some degree, LV reverse remodeling. Moreover, several electrical and imaging parameters might aid proper selection and stratification of HCM patients to benefit from CRT. Nonetheless, current available data are scarce and further studies are still required to accurately clarify the view. This review reassesses the importance of CRT in patients with HCM based on current research by contrasting and contextualizing data from various published studies.
Keywords: apical rocking; cardiac resynchronization therapy; end-stage/dilated hypertrophic cardiomyopathy; hypertrophic cardiomyopathy; left bundle branch block.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Glikson M., Nielsen J.C., Kronborg M.B., Michowitz Y., Auricchio A., Barbash I.M., Barrabés J.A., Boriani G., Braunschweig F., Brignole M., et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021;42:3427–3520. doi: 10.1093/eurheartj/ehab364. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
