

Transfer of Cardiac Mitochondria Improves the Therapeutic Efficacy of Mesenchymal Stem Cells in a Preclinical Model of Ischemic Heart Disease
- PMID: 36831249
- PMCID: PMC9953768
- DOI: 10.3390/cells12040582
Transfer of Cardiac Mitochondria Improves the Therapeutic Efficacy of Mesenchymal Stem Cells in a Preclinical Model of Ischemic Heart Disease
Abstract
Background: The use of mesenchymal stem cells (MSCs) appears to be a promising therapeutic approach for cardiac repair after myocardial infarction. However, clinical trials have revealed the need to improve their therapeutic efficacy. Recent evidence demonstrated that mitochondria undergo spontaneous transfer from damaged cells to MSCs, resulting in the activation of the cytoprotective and pro-angiogenic functions of recipient MSCs. Based on these observations, we investigated whether the preconditioning of MSCs with mitochondria could optimize their therapeutic potential for ischemic heart disease.
Methods: Human MSCs were exposed to mitochondria isolated from human fetal cardiomyocytes. After 24 h, the effects of mitochondria preconditioning on the MSCs' function were analyzed both in vitro and in vivo.
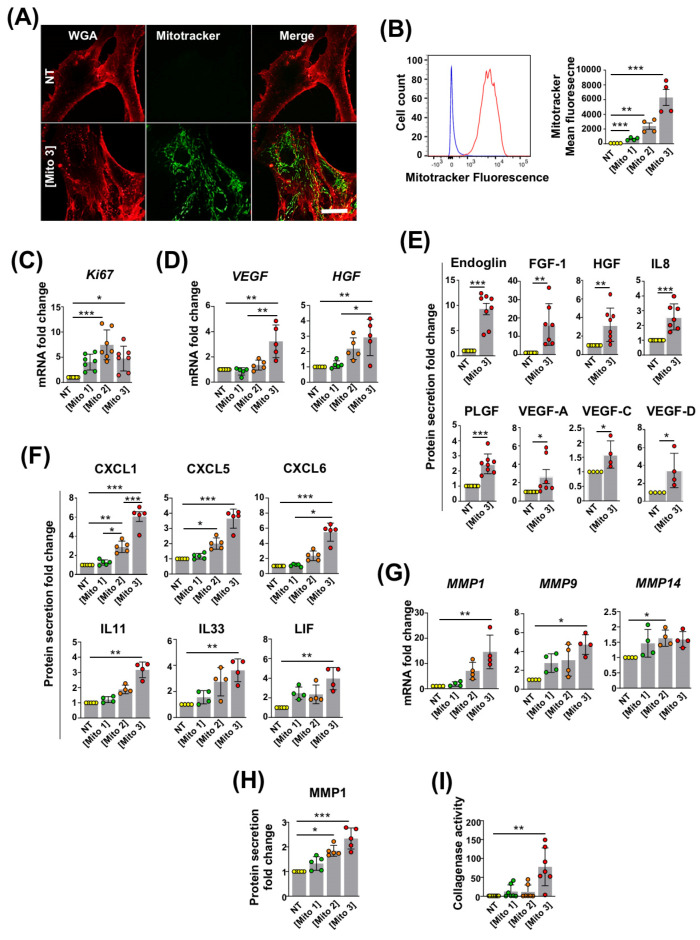
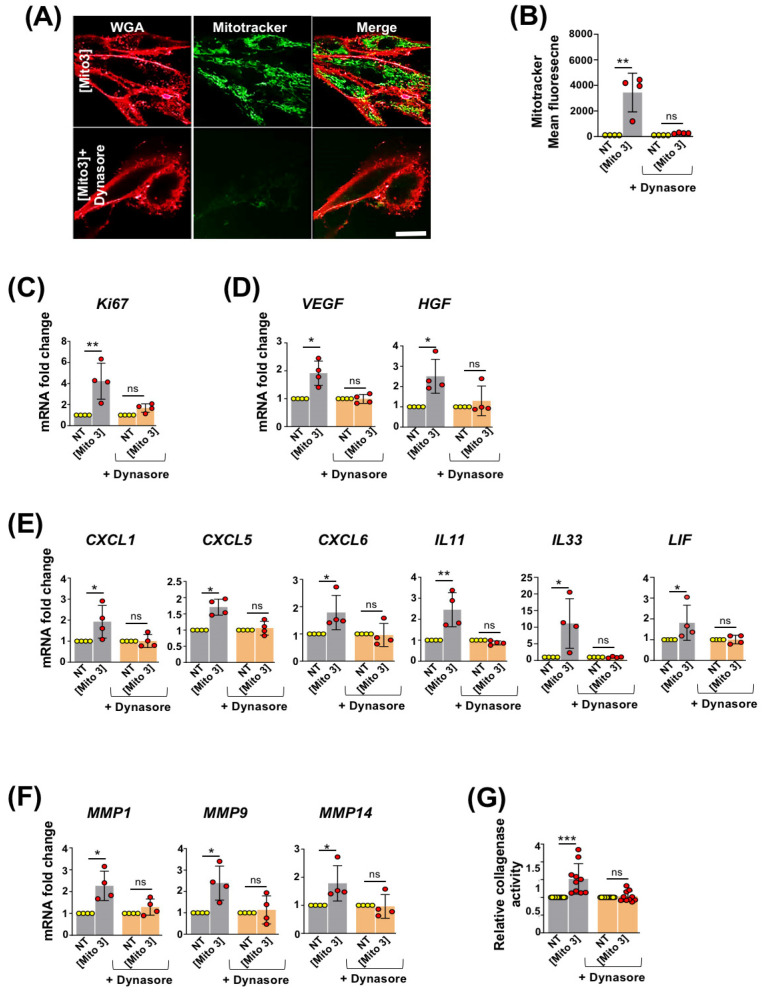
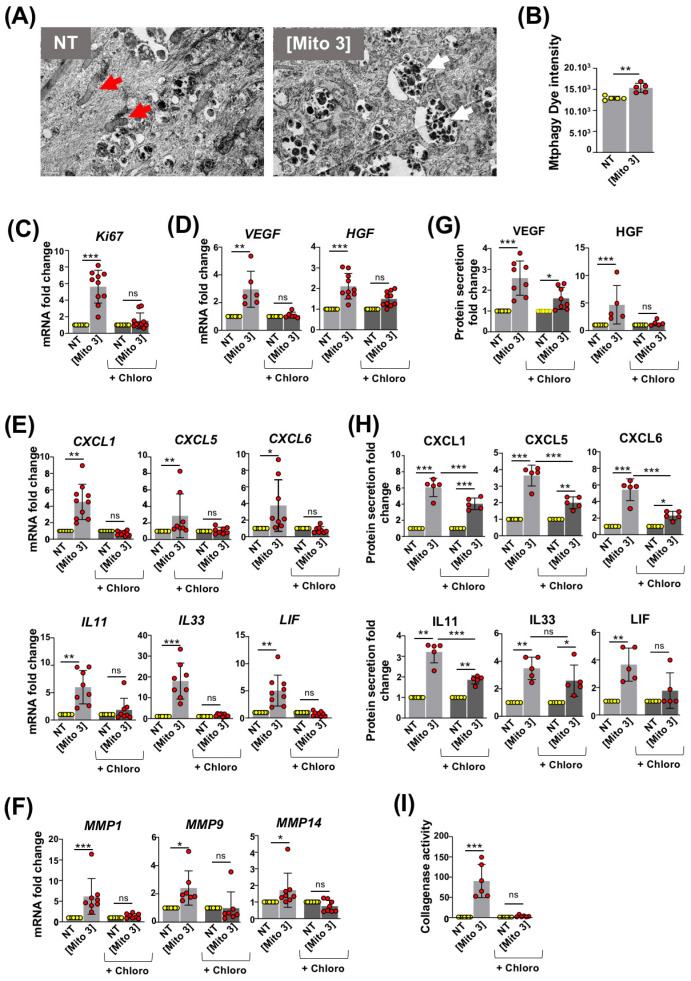
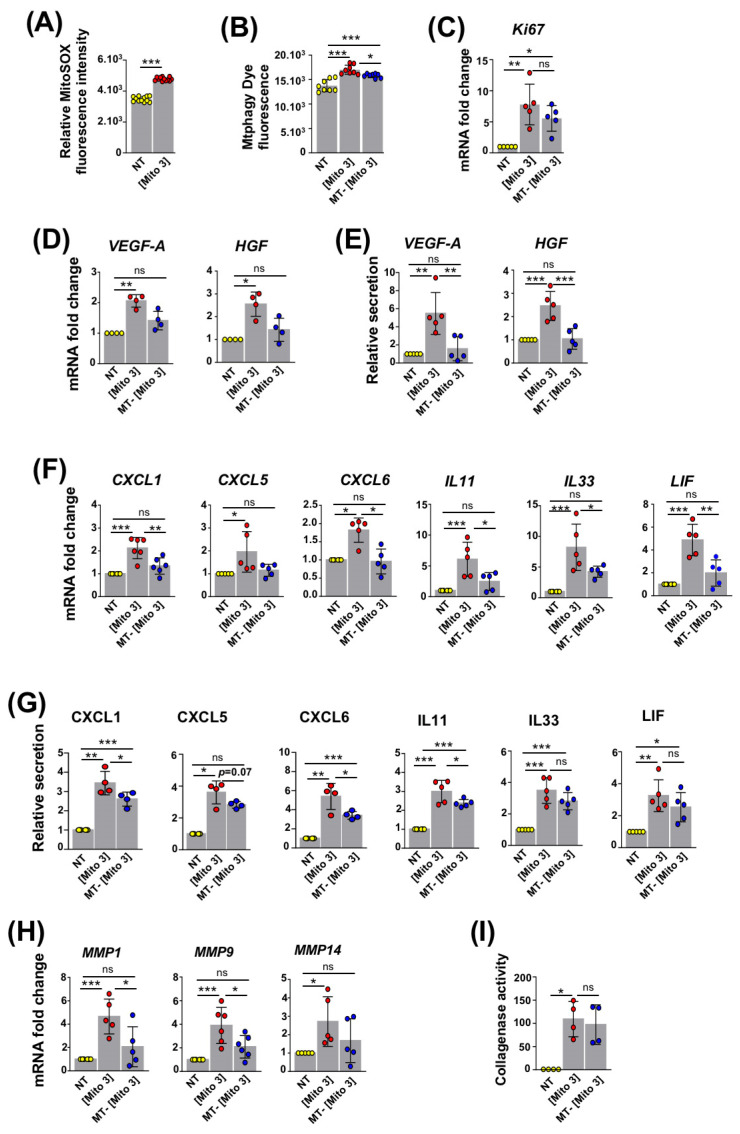
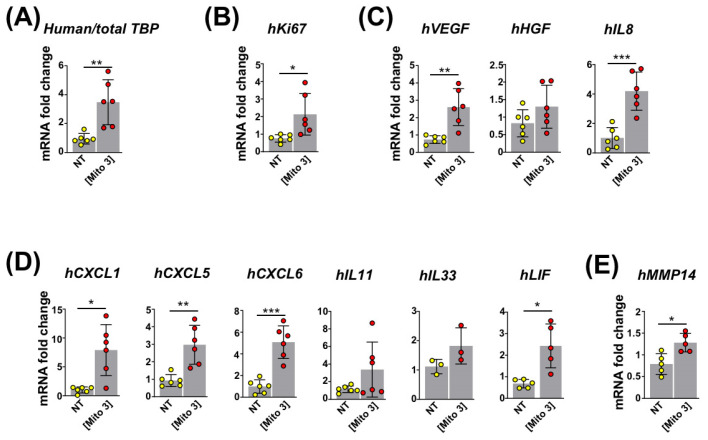
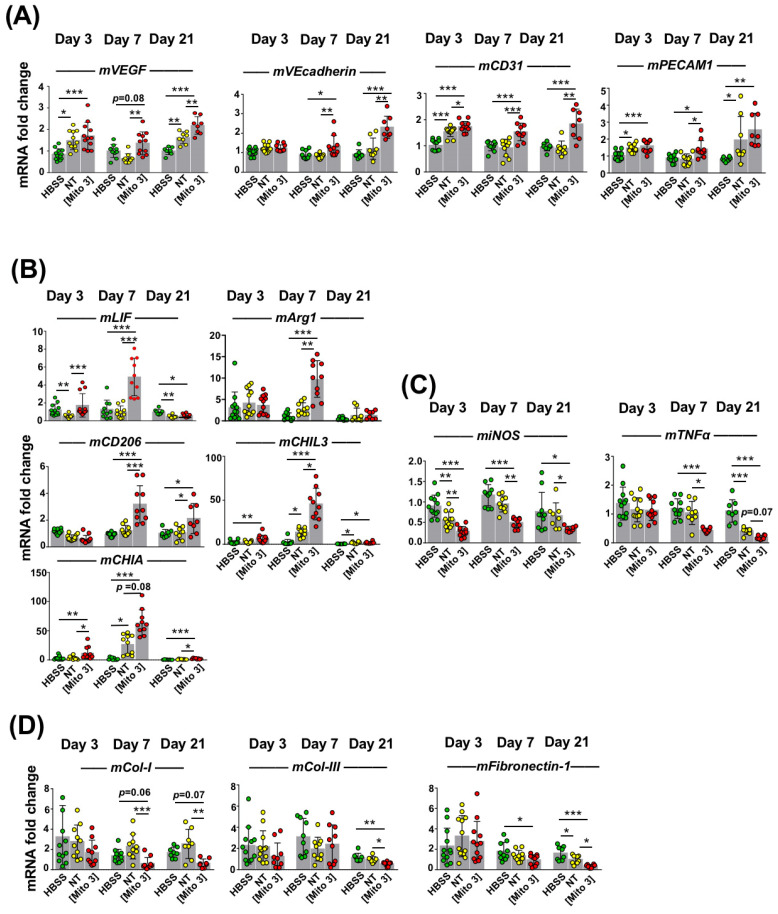
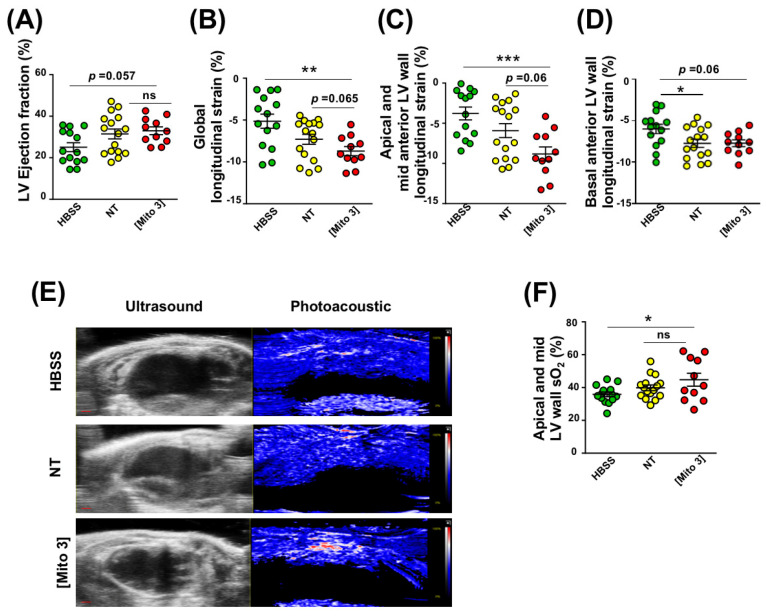
Results: We found that cardiac mitochondria-preconditioning improved the proliferation and repair properties of MSCs in vitro. Mechanistically, cardiac mitochondria mediate their stimulatory effects through the production of reactive oxygen species, which trigger their own degradation in recipient MSCs. These effects were further confirmed in vivo, as the mitochondria preconditioning of MSCs potentiated their therapeutic efficacy on cardiac function following their engraftment into infarcted mouse hearts.
Conclusions: The preconditioning of MSCs with the artificial transfer of cardiac mitochondria appears to be promising strategy to improve the efficacy of MSC-based cell therapy in ischemic heart disease.
Keywords: cell therapy; mesenchymal stem cells; metabolism; mitochondria transfer; post-ischemic heart failure.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Agbulut O., Mazo M., Bressolle C., Gutierrez M., Azarnoush K., Sabbah L., Niederlander N., Abizanda G., Andreu E.J., Pelacho B., et al. Can bone marrow-derived multipotent adult progenitor cells regenerate infarcted myocardium? Cardiovasc. Res. 2006;72:175–183. doi: 10.1016/j.cardiores.2006.07.009. - DOI - PubMed
-
- Hamdi H., Planat-Benard V., Bel A., Puymirat E., Geha R., Pidial L., Nematalla H., Bellamy V., Bouaziz P., Peyrard S., et al. Epicardial adipose stem cell sheets results in greater post-infarction survival than intramyocardial injections. Cardiovasc. Res. 2011;91:483–491. doi: 10.1093/cvr/cvr099. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
