

Prognosis of Pancreatic Cancer Based on Resectability: A Single Center Experience
- PMID: 36831444
- PMCID: PMC9954753
- DOI: 10.3390/cancers15041101
Prognosis of Pancreatic Cancer Based on Resectability: A Single Center Experience
Abstract
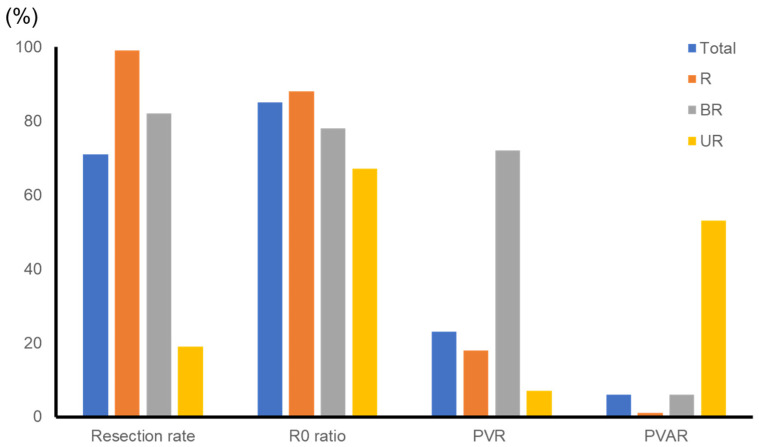
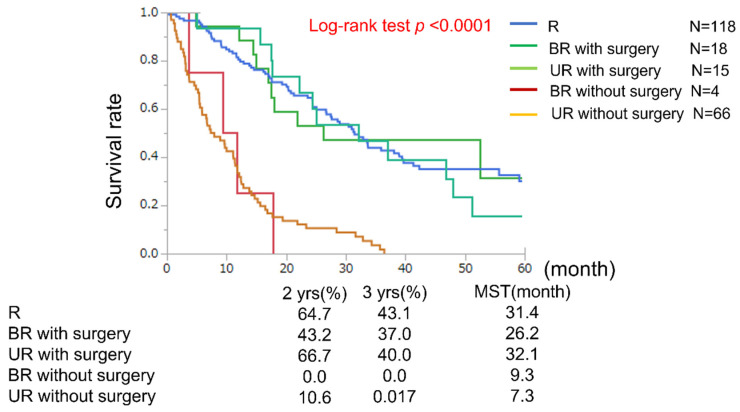
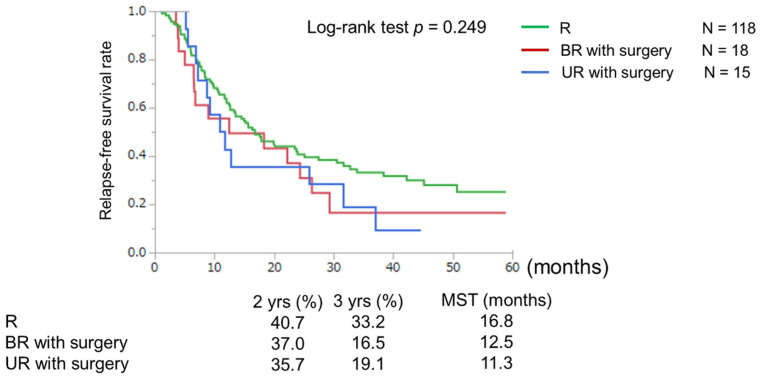
Although conversion surgery has increasingly been performed for initially unresectable advanced pancreatic ductal adenocarcinoma (PDAC), the rate of conversion, including that for patients who do not undergo resection, remains unclear. Patients with PDAC who were treated between January 2013 and December 2018 were classified into three groups: resectable (R), borderline resectable (BR), and unresectable (UR). We analyzed patient outcomes, including the rate of surgical resection and survival, in each of these groups. In total, 211 patients (R, 118; BR, 22; UR, 81) were selected. Among them, 117 (99%), 18 (82%), and 15 (19%) patients in the R, BR, and UR groups, respectively, underwent surgical resection. R0 resection rates were 88, 78, and 67%, whereas median overall survival (OS) from treatment initiation were 31, 18, and 11 months (p < 0.0001) in the R, BR, and UR groups, respectively. In patients who underwent surgical resection, relapse-free survival (RFS) and OS were similar among the three groups (R vs. BR vs. UR; median RFS (months), 17 vs. 13 vs. 11, p = 0.249; median OS (months), 31 vs. 26 vs. 32, p = 0.742). Lymph node metastases and incomplete adjuvant chemotherapy were identified as independent prognostic factors for OS. Although the surgical resection rate was low, particularly in the BR and UR groups, the prognosis of patients who underwent surgical resection was similar irrespective of the initial resectability status.
Keywords: conversion surgery; pancreatic cancer; resectability.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Fujii T., Sugimoto H., Yamada S., Kanda M., Suenaga M., Takami H., Hattori M., Inokawa Y., Nomoto S., Fujiwara M., et al. Modified Blumgart anastomosis for pancreaticojejunostomy: Technical improvement in matched historical control study. J. Gastrointest. Surg. 2014;18:1108–1115. doi: 10.1007/s11605-014-2523-3. - DOI - PubMed
-
- Fujii T., Yamada S., Murotani K., Kanda M., Sugimoto H., Nakao A., Kodera Y. Inverse Probability of Treatment Weighting Analysis of Upfront Surgery Versus Neoadjuvant Chemoradiotherapy Followed by Surgery for Pancreatic Adenocarcinoma with Arterial Abutment. Medicine. 2015;94:e1647. doi: 10.1097/MD.0000000000001647. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
