

Evaluating the Risk of Inguinal Lymph Node Metastases before Surgery Using the Morphonode Predictive Model: A Prospective Diagnostic Study in Vulvar Cancer Patients
- PMID: 36831462
- PMCID: PMC9953890
- DOI: 10.3390/cancers15041121
Evaluating the Risk of Inguinal Lymph Node Metastases before Surgery Using the Morphonode Predictive Model: A Prospective Diagnostic Study in Vulvar Cancer Patients
Abstract
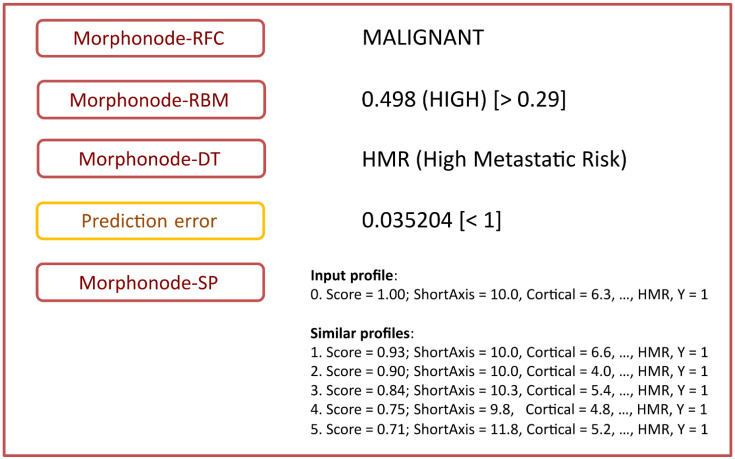
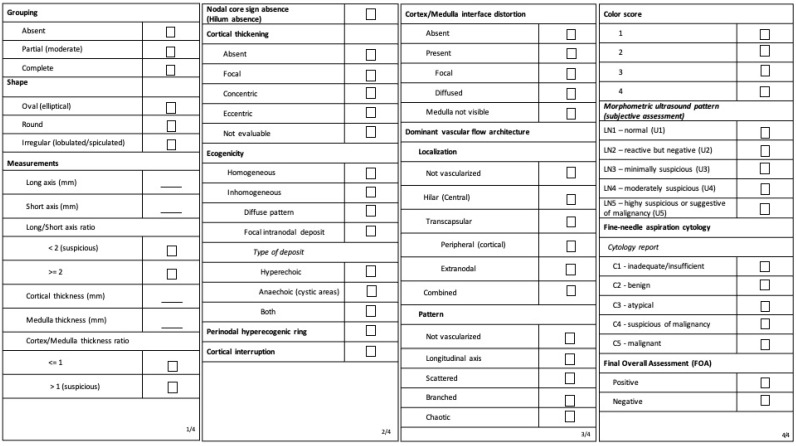
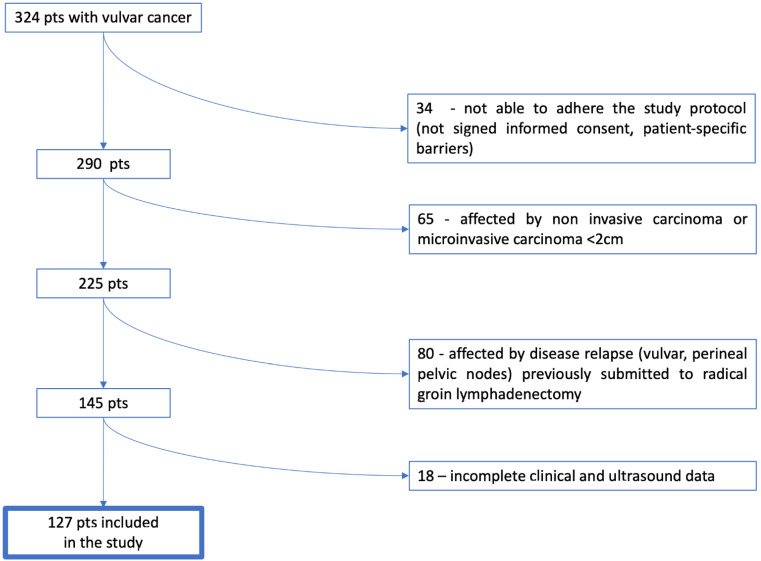
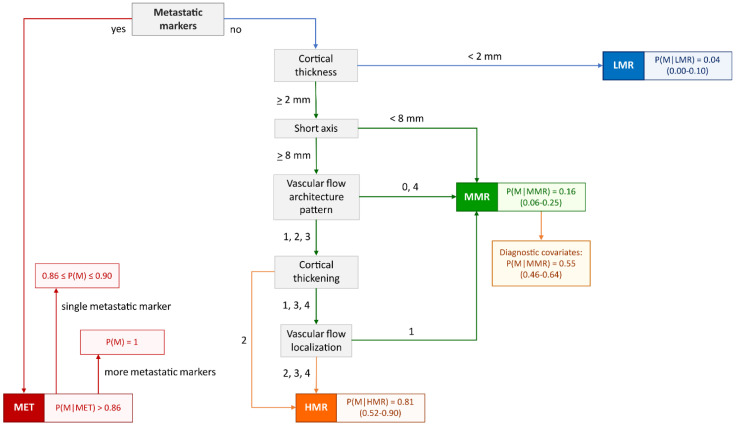
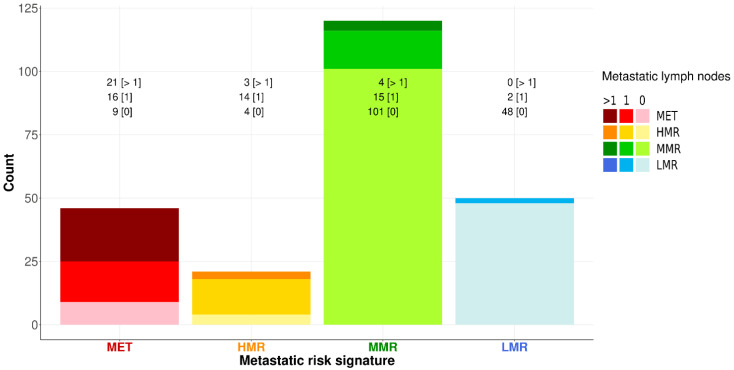
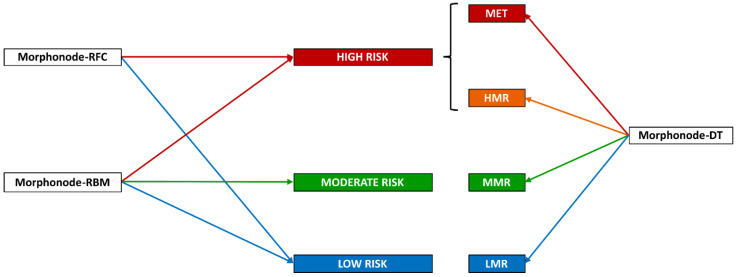
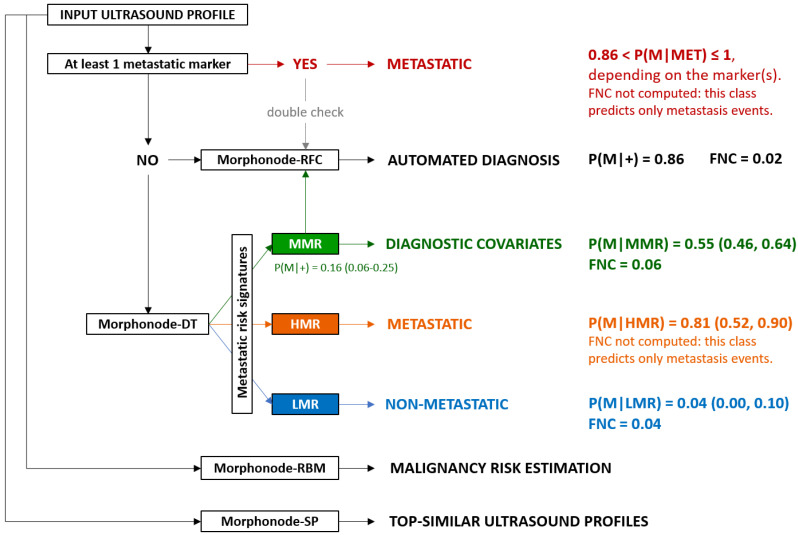
Ultrasound examination is an accurate method in the preoperative evaluation of the inguinofemoral lymph nodes when performed by experienced operators. The purpose of the study was to build a robust, multi-modular model based on machine learning to discriminate between metastatic and non-metastatic inguinal lymph nodes in patients with vulvar cancer. One hundred and twenty-seven women were selected at our center from March 2017 to April 2020, and 237 inguinal regions were analyzed (75 were metastatic and 162 were non-metastatic at histology). Ultrasound was performed before surgery by experienced examiners. Ultrasound features were defined according to previous studies and collected prospectively. Fourteen informative features were used to train and test the machine to obtain a diagnostic model (Morphonode Predictive Model). The following data classifiers were integrated: (I) random forest classifiers (RCF), (II) regression binomial model (RBM), (III) decisional tree (DT), and (IV) similarity profiling (SP). RFC predicted metastatic/non-metastatic lymph nodes with an accuracy of 93.3% and a negative predictive value of 97.1%. DT identified four specific signatures correlated with the risk of metastases and the point risk of each signature was 100%, 81%, 16% and 4%, respectively. The Morphonode Predictive Model could be easily integrated into the clinical routine for preoperative stratification of vulvar cancer patients.
Keywords: lymph nodes; machine learning; ultrasound; vulvar cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Ultrasound morphometric and cytologic preoperative assessment of inguinal lymph-node status in women with vulvar cancer: MorphoNode study.Ultrasound Obstet Gynecol. 2020 Mar;55(3):401-410. doi: 10.1002/uog.20378. Ultrasound Obstet Gynecol. 2020. PMID: 31237047
-
Ultrasound-guided FNA cytology of groin lymph nodes improves the management of squamous cell carcinoma of the vulva: Results from a comparative cytohistological study.Cancer Cytopathol. 2019 Aug;127(8):514-520. doi: 10.1002/cncy.22154. Epub 2019 Jun 7. Cancer Cytopathol. 2019. PMID: 31174235
-
The role of preoperative ultrasound evaluation of inguinal lymph nodes in patients with vulvar malignancy.Gynecol Oncol. 2013 Oct;131(1):113-7. doi: 10.1016/j.ygyno.2013.07.103. Epub 2013 Aug 7. Gynecol Oncol. 2013. PMID: 23932893
-
The Role of Ultrasound in the Evaluation of Inguinal Lymph Nodes in Patients with Vulvar Cancer: A Systematic Review and Meta-Analysis.Cancers (Basel). 2022 Jun 23;14(13):3082. doi: 10.3390/cancers14133082. Cancers (Basel). 2022. PMID: 35804853 Free PMC article. Review.
-
Management of the lymph nodes in penile cancer.Urology. 2010 Aug;76(2 Suppl 1):S43-57. doi: 10.1016/j.urology.2010.03.001. Urology. 2010. PMID: 20691885 Review.
Cited by
-
Machine Learning Based Assessment of Inguinal Lymph Node Metastasis in Patients with Squamous Cell Carcinoma of the Vulva.J Clin Med. 2025 May 17;14(10):3510. doi: 10.3390/jcm14103510. J Clin Med. 2025. PMID: 40429505 Free PMC article.
-
Application of artificial intelligence to ultrasound imaging for benign gynecological disorders: systematic review.Ultrasound Obstet Gynecol. 2025 Mar;65(3):295-302. doi: 10.1002/uog.29171. Epub 2025 Jan 31. Ultrasound Obstet Gynecol. 2025. PMID: 39888598 Free PMC article.
-
Current Preoperative Management of Vulvar Squamous Cell Carcinoma: An Overview.Cancers (Basel). 2024 May 11;16(10):1846. doi: 10.3390/cancers16101846. Cancers (Basel). 2024. PMID: 38791925 Free PMC article. Review.
References
-
- Land R., Herod J., Moskovic E., King M., Sohaib S.A., Trott P., Nasiri N., Shepherd J.H., Bridges J.E., Ind T.E., et al. Routine Computerized Tomography Scanning, Groin Ultrasound with or without Fine Needle Aspiration Cytology in the Surgical Management of Primary Squamous Cell Carcinoma of the Vulva. Int. J. Gynecol. Cancer. 2006;16:312–317. doi: 10.1111/j.1525-1438.2006.00340.x. - DOI - PubMed
-
- Gui B., Persiani S., Miccò M., Pignatelli V., Rodolfino E., Avesani G., Di Paola V., Panico C., Russo L., Fragomeni S.M., et al. MRI Staging in Locally Advanced Vulvar Cancer: From Anatomy to Clinico-Radiological Findings. A Multidisciplinary VulCan Team Point of View. J. Pers. Med. 2021;11:1219. doi: 10.3390/jpm11111219. - DOI - PMC - PubMed
-
- Oonk M.H.M., Planchamp F., Baldwin P., Bidzinski M., Brännström M., Landoni F., Mahner S., Mahantshetty U., Mirza M., Petersen C., et al. European Society of Gynaecological Oncology Guidelines for the Management of Patients with Vulvar Cancer. Int. J. Gynecol. Cancer. 2017;27:832–837. doi: 10.1097/IGC.0000000000000975. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
