

Breast Cancer Risk Assessment Tools for Stratifying Women into Risk Groups: A Systematic Review
- PMID: 36831466
- PMCID: PMC9953796
- DOI: 10.3390/cancers15041124
Breast Cancer Risk Assessment Tools for Stratifying Women into Risk Groups: A Systematic Review
Abstract
Background: The benefits and harms of breast screening may be better balanced through a risk-stratified approach. We conducted a systematic review assessing the accuracy of questionnaire-based risk assessment tools for this purpose.
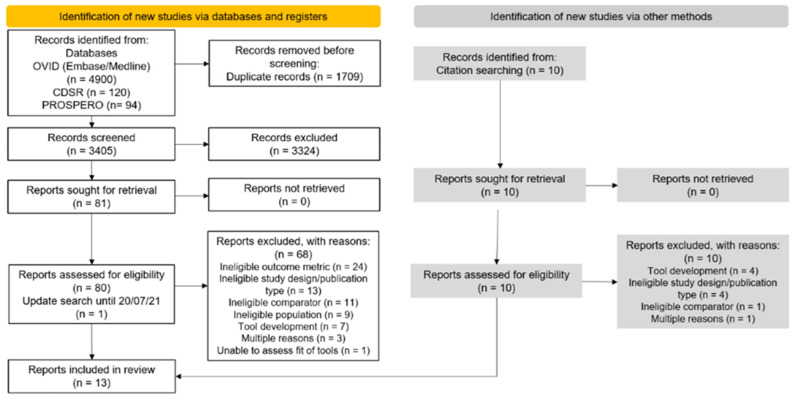
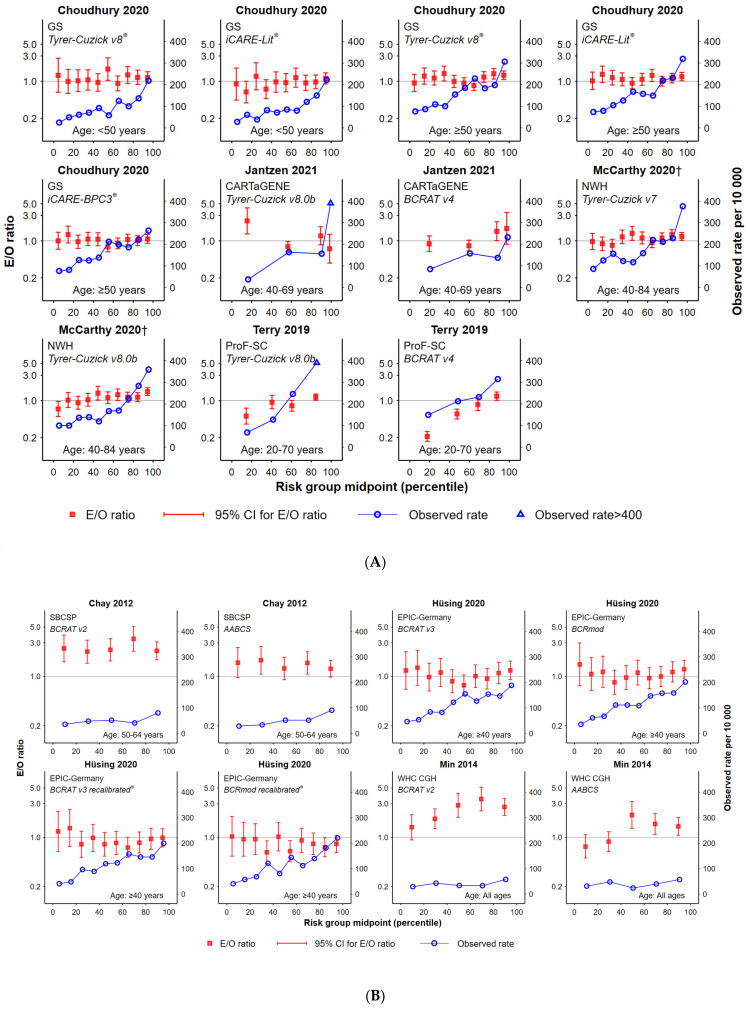
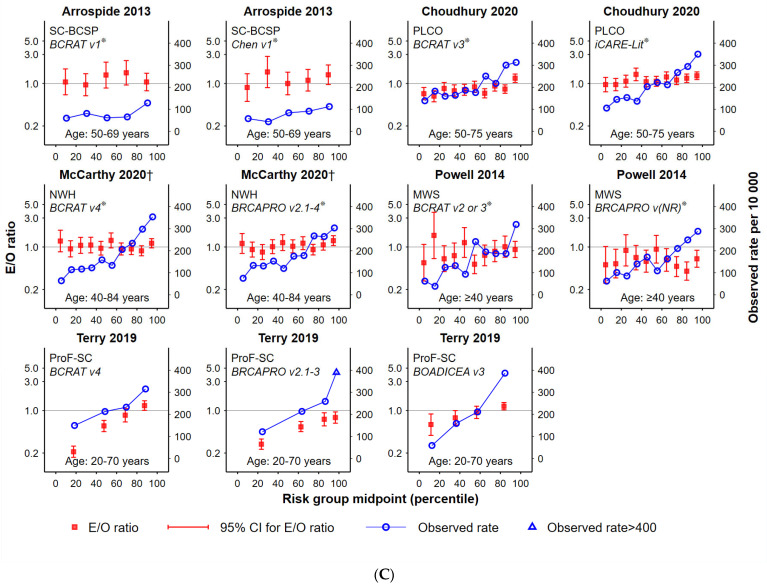
Methods: Population: asymptomatic women aged ≥40 years; Intervention: questionnaire-based risk assessment tool (incorporating breast density and polygenic risk where available); Comparison: different tool applied to the same population; Primary outcome: breast cancer incidence; Scope: external validation studies identified from databases including Medline and Embase (period 1 January 2008-20 July 2021). We assessed calibration (goodness-of-fit) between expected and observed cancers and compared observed cancer rates by risk group. Risk of bias was assessed with PROBAST.
Results: Of 5124 records, 13 were included examining 11 tools across 15 cohorts. The Gail tool was most represented (n = 11), followed by Tyrer-Cuzick (n = 5), BRCAPRO and iCARE-Lit (n = 3). No tool was consistently well-calibrated across multiple studies and breast density or polygenic risk scores did not improve calibration. Most tools identified a risk group with higher rates of observed cancers, but few tools identified lower-risk groups across different settings. All tools demonstrated a high risk of bias.
Conclusion: Some risk tools can identify groups of women at higher or lower breast cancer risk, but this is highly dependent on the setting and population.
Keywords: breast cancer screening; risk assessment; risk prediction models; risk-based screening.
Conflict of interest statement
LSV, VF and DC have received salary support via the grant from the Australian Government, Department of Health (see funding section) paid to their institution. CN leads the ROSA project which has received the above-named funding.
Figures
References
-
- Schünemann H.J., Lerda D., Quinn C., Follmann M., Alonso-Coello P., Rossi P.G., Lebeau A., Nyström L., Broeders M., Ioannidou-Mouzaka L., et al. European Commission Initiative on Breast Cancer (ECIBC) Contributor Group. Breast Cancer Screening and Diagnosis: A Synopsis of the European Breast Guidelines. Ann. Intern. Med. 2020;172:46–56. doi: 10.7326/M19-2125. - DOI - PubMed
-
- Monticciolo D.L., Newell M.S., Hendrick R.E., Helvie M.A., Moy L., Monsees B., Kopans D.B., Eby P.R., Sickles E.A. Breast Cancer Screening for Average-Risk Women: Recommendations from the ACR Commission on Breast Imaging. J. Am. Coll. Radiol. 2017;14:1137–1143. - PubMed
-
- Siu A.L., U.S. Preventive Services Task Force Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2016;164:279–296. - PubMed
-
- Elder K., Nickson C., Pattanasri M., Cooke S., Machalek D., Rose A., Mou A., Collins J.P., Park A., De Boer R., et al. Treatment intensity differences after early-stage breast cancer (ESBC) diagnosis depending on participation in a screening program. Ann. Surg. Oncol. 2018;25:2563–2572. doi: 10.1245/s10434-018-6469-7. - DOI - PubMed
-
- Nelson H.D., Pappas M., Cantor A., Griffin J., Daeges M., Humphrey L. Harms of Breast Cancer Screening: Systematic Review to Update the 2009 U.S. Preventive Services Task Force Recommendation. Ann. Intern. Med. 2016;164:256–267. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
