

Early Hospital Discharge on Day Two Post Robotic Lobectomy with Telehealth Home Monitoring: A Pilot Study
- PMID: 36831489
- PMCID: PMC9954553
- DOI: 10.3390/cancers15041146
Early Hospital Discharge on Day Two Post Robotic Lobectomy with Telehealth Home Monitoring: A Pilot Study
Abstract
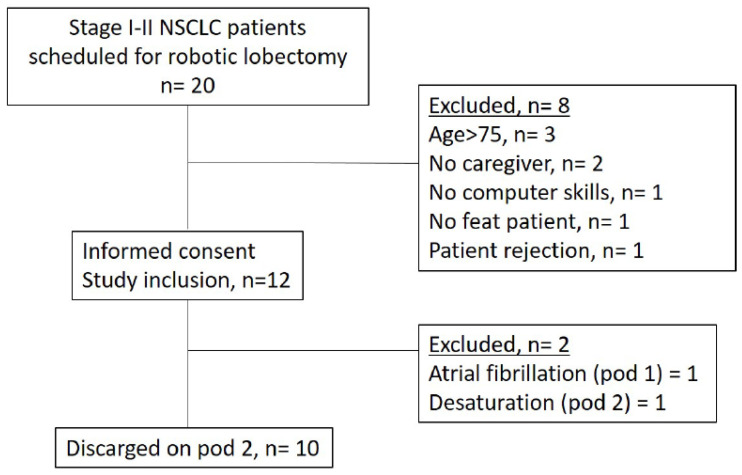
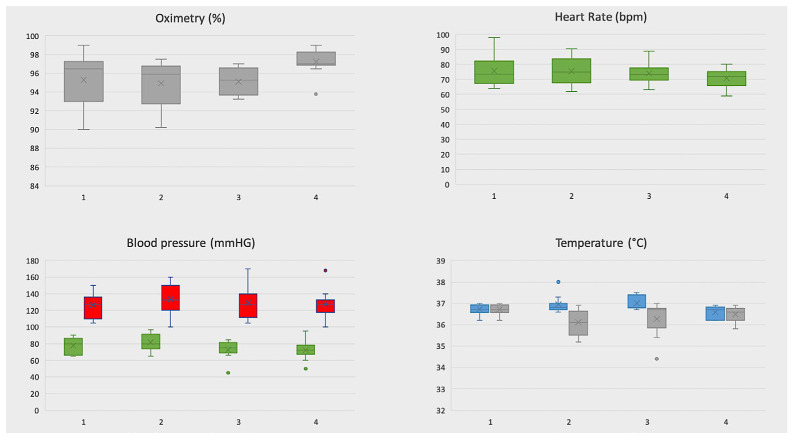
Despite the adoption of enhanced recovery programs, the reported postoperative length of stay after robotic surgery is 4 days even in highly specialized centers. We report preliminary results of a pilot study for a new protocol of early discharge (on day 2) with telehealth home monitoring after robotic lobectomy for lung cancer. All patients with a caregiver were discharged on postoperative day 2 with a telemonitoring device if they satisfied specific discharge criteria. Teleconsultations were scheduled once in the afternoon of post-operative day 2, twice on postoperative day 3, and then once a day until the chest tube removal. Post-discharge vital signs were recorded by patients at least four times daily through the device and were available for consultation by two surgeons through phone application. In case of sudden variation of vital signs or occurrence of adverse events, a direct telephone line was available for patients as well as a protected re-hospitalization path. Primary outcome was the safety evaluated by the occurrence of post-discharge complications and readmissions. Secondary outcome was the evaluation of resources optimization (hospitalization days) maintaining the standard of care. During the study period, twelve patients satisfied all preoperative clinical criteria to be enrolled in our protocol. Two of twelve enrolled patients were successively excluded because they did not satisfy discharge criteria on postoperative day 2. During telehealth home monitoring a total of 27/427 vital-sign measurements violated the threshold in seven patients. Among the threshold violations, only 1 out of 27 was a critical violation and was managed at home. No postoperative complication occurred neither readmission was needed. A mean number of three hospitalization days was avoided and an estimated economic benefit of about EUR 500 for a single patient was obtained if compared with patients submitted to VATS lobectomy in the same period. These preliminary results confirm that adoption of telemonitoring allows, in selected patients, a safe discharge on postoperative day 2 after robotic surgery for early-stage NSCLC. A potential economic benefit could derive from this protocol if this data will be confirmed in larger sample.
Keywords: NSCLC; early discharge; lung cancer; oncological surgery; tele monitoring; telehealth home monitoring thoracic surgery; telemedicine.
Conflict of interest statement
E. Bottoni has received honoraria from AB Medica SpA. The other authors have no conflict of interest to declare with respect to research, authorship, and/or publication of this article.
Figures
References
-
- Falcoz P.-E., Puyraveau M., Thomas P., Decaluwe H., Hürtgen M., Petersen R.H., Hansen H., Brunelli A., Van Raemdonck D., Dahan M., et al. Video-assisted thoracoscopic surgery versus open lobectomy for primary non-small-cell lung cancer: A propensity-matched analysis of outcome from the European Society of Thoracic Surgeon database. Eur. J. Cardio-Thorac. Surg. 2015;49:602–609. doi: 10.1093/ejcts/ezv154. - DOI - PubMed
-
- Batchelor T.J.P., Rasburn N.J., Abdelnour-Berchtold E., Brunelli A., Cerfolio R.J., Gonzalez M., Ljungqvist O., Petersen R.H., Popescu W.M., Slinger P.D., et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery After Surgery (ERASVR) Society and the European Society of Thoracic Surgeons (ESTS) Eur. J. Cardiothorac Surg. 2019;55:91–115. doi: 10.1093/ejcts/ezy301. - DOI - PubMed
-
- Patel Y.S., Hanna W.C., Fahim C., Shargall Y., Waddell T.K., Yasufuku K., Machuca T.N., Pipkin M., Baste J.-M., Xie F., et al. RAVAL trial: Protocol of an international, multi-centered, blinded, randomized controlled trial comparing robotic-assisted versus video-assisted lobectomy for early-stage lung cancer. PLoS ONE. 2022;17:e0261767. doi: 10.1371/journal.pone.0261767. - DOI - PMC - PubMed
