

New Challenges in the Management of Cholangiocarcinoma: The Role of Liver Transplantation, Locoregional Therapies, and Systemic Therapy
- PMID: 36831586
- PMCID: PMC9953927
- DOI: 10.3390/cancers15041244
New Challenges in the Management of Cholangiocarcinoma: The Role of Liver Transplantation, Locoregional Therapies, and Systemic Therapy
Abstract
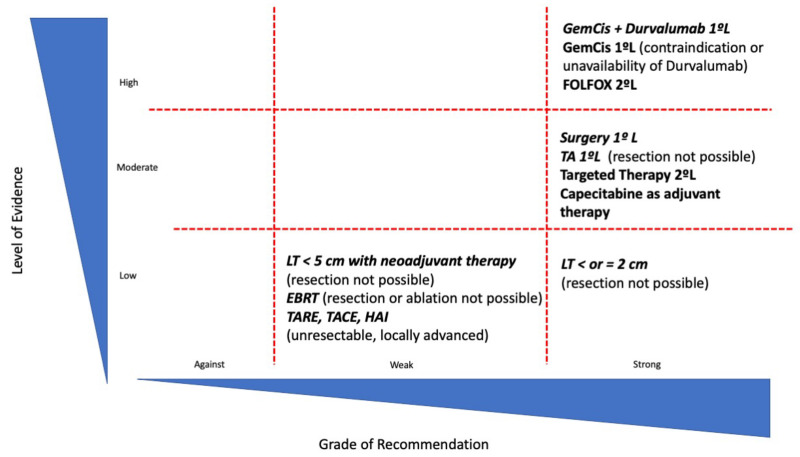
Cholangiocarcinoma (CCA) is a neoplasm with high mortality that represents 15% of all primary liver tumors. Its worldwide incidence is on the rise, and despite important advances in the knowledge of molecular mechanisms, diagnosis, and treatment, overall survival has not substantially improved in the last decade. Surgical resection remains the cornerstone therapy for CCA. Unfortunately, complete resection is only possible in less than 15-35% of cases, with a risk of recurrence greater than 60%. Liver transplantation (LT) has been postulated as an effective therapeutic strategy in those intrahepatic CCA (iCCA) smaller than 3 cm. However, the low rate of early diagnosis in non-resectable patients justifies the low applicability in clinical practice. The evidence regarding LT in locally advanced iCCA is scarce and based on small, retrospective, and, in most cases, single-center case series. In this setting, the response to neoadjuvant chemotherapy could be useful in identifying a subgroup of patients with biologically less aggressive tumors in whom LT may be successful. The results of LT in pCCA are promising, however, we need a very careful selection of patients and adequate experience in the transplant center. Locoregional therapies may be relevant in unresectable, liver-only CCA. In iCCA smaller than 2 cm, particularly those arising in patients with advanced chronic liver disease in whom resection or LT may not be feasible, thermal ablation may become a reliable alternative. The greatest advances in the management of CCA occur in systemic treatment. Immunotherapy associated with chemotherapy has emerged as the gold standard in the first-line treatment. Likewise, the most encouraging results have been obtained with targeted therapies, where the use of personalized treatments has shown high rates of objective and durable tumor response, with clear signs of survival benefit. In conclusion, the future of CCA treatment seems to be marked by the development of new treatment strategies but high-quality, prospective studies that shed light on their use and applicability are mandatory.
Keywords: cholangiocarcinoma; liver transplant; locoregional therapies; systemic treatment.
Conflict of interest statement
E. Mauro: Received speaker fees from Roche and Sirtex, and travel funding from MSD. J. Ferrer-Fàbrega: Received lecture fees from Bayer and Astrazeneca and consultancy fees from Astrazeneca. T. Sauri: None. A. Soler: None. A. Cobo: None. M. Burrel: None. G. Iserte: Received travel expenses from Bayer. A. Forner: Received lecture fees from Gilead, Boston Scientific, and MSD, as well as consultancy fees from Bayer, AstraZeneca, Roche, SIRTEX, AB Exact Science, and Guerbert.
Figures
References
-
- Banales J.M., Marin J.J.G., Lamarca A., Rodrigues P.M., Khan S.A., Roberts L.R., Cardinale V., Carpino G., Andersen J.B., Braconi C., et al. Cholangiocarcinoma 2020: The next Horizon in Mechanisms and Management. Nat. Rev. Gastroenterol. Hepatol. 2020;17:557–588. doi: 10.1038/s41575-020-0310-z. - DOI - PMC - PubMed
-
- Izquierdo-Sanchez L., Lamarca A., la Casta A., Buettner S., Utpatel K., Klümpen H.-J., Adeva J., Vogel A., Lleo A., Fabris L., et al. Cholangiocarcinoma Landscape in Europe: Diagnostic, Prognostic and Therapeutic Insights from the ENSCCA Registry. J. Hepatol. 2022;76:1109–1121. doi: 10.1016/j.jhep.2021.12.010. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
