

Diametaphyseal Distal Forearm Fractures in Children: A STROBE Compliant Comparison of Outcomes of Different Stabilization Techniques Regarding Complications
- PMID: 36832503
- PMCID: PMC9955196
- DOI: 10.3390/children10020374
Diametaphyseal Distal Forearm Fractures in Children: A STROBE Compliant Comparison of Outcomes of Different Stabilization Techniques Regarding Complications
Abstract
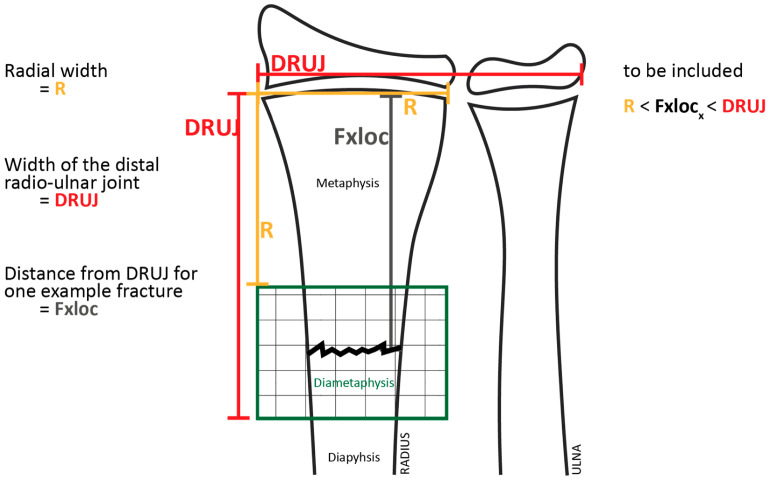
Diametaphyseal forearm fractures are difficult to treat because standard methods for long-bone fracture stabilization in the metaphyseal or diaphyseal regions are less effective in this transition zone. We hypothesized that there is no difference in outcomes between conservative and surgical treatment of diametaphyseal forearm fractures. This retrospective analysis included 132 patients who had undergone treatment for diametaphyseal forearm fracture between 2013 and 2020 at our institution. The primary analysis compared complications occurring in patients treated conservatively with those occurring in patients managed surgically (ESIN, K-wire fixation, KESIN stabilization, or open reduction and plate osteosynthesis). In a subgroup analysis, we compared the two most frequently applied surgical stabilization techniques in distal forearm fractures (i.e., ESIN and K-wire) with conservative treatment. The mean age of the patients at the time of intervention was 9.43 ± 3.78 years (mean ± SD). Most patients were male (91; 68.9%), and 70 of 132 (53.1%) patients underwent surgical stabilization. The rate of re-intervention or complications was similar after conservative and surgical treatment, and ESIN or K-wire fixation achieved comparable complication rates. Recurrent displacement of fragments was the most frequent reason for re-interventions (13 of 15 patients; 86.6%). There was no permanent damage as a result of a complication. The median time of exposure to image intensifier radiation was comparable between ESIN (95.5 s) and K-wire fixation (85.0 s), but significantly lower during conservative treatment (15.0 s; p = 0.001).
Keywords: ESIN; K-wire; diametaphyseal fracture; distal radius; pediatric trauma.
Conflict of interest statement
We report no conflict of interest.
Figures





Similar articles
-
Therapeutic approaches of diametaphyseal radius fractures in children.Arch Orthop Trauma Surg. 2024 Mar;144(3):1179-1188. doi: 10.1007/s00402-023-05118-z. Epub 2024 Jan 17. Arch Orthop Trauma Surg. 2024. PMID: 38231205
-
Is there a standard treatment for displaced pediatric diametaphyseal forearm fractures?: A STROBE-compliant retrospective study.Medicine (Baltimore). 2019 Jul;98(28):e16353. doi: 10.1097/MD.0000000000016353. Medicine (Baltimore). 2019. PMID: 31305426 Free PMC article.
-
Unstable diametaphyseal forearm fractures: transepiphyseal intramedullary Kirschner-wire fixation as a treatment option in children.Eur J Pediatr Surg. 2010 Nov;20(6):395-8. doi: 10.1055/s-0030-1262843. Epub 2010 Oct 11. Eur J Pediatr Surg. 2010. PMID: 20938899
-
[Diametaphyseal forearm fracture in childhood. Pitfalls and recommendations for treatment].Unfallchirurg. 2011 Apr;114(4):292-9. doi: 10.1007/s00113-011-1962-5. Unfallchirurg. 2011. PMID: 21445651 Review. German.
-
Displaced distal radius fractures in children, cast alone vs additional K-wire fixation: a meta-analysis.Eur J Trauma Emerg Surg. 2019 Dec;45(6):1003-1011. doi: 10.1007/s00068-018-1011-y. Epub 2018 Oct 1. Eur J Trauma Emerg Surg. 2019. PMID: 30276723 Free PMC article.
Cited by
-
Clinical Outcomes of Minimally Invasive Fixation with Pre-Bent Elastic Stable Intramedullary Nails for the Treatment of Distal Radius Metaphyseal Diaphysis Junction Fractures in Children.Orthop Surg. 2023 Dec;15(12):3223-3230. doi: 10.1111/os.13919. Epub 2023 Oct 25. Orthop Surg. 2023. PMID: 37880202 Free PMC article.
-
Healing smarter: A systematic review and meta-analysis of bioresorbable implants for paediatric forearm fractures.J Child Orthop. 2025 Aug 19:18632521251350854. doi: 10.1177/18632521251350854. Online ahead of print. J Child Orthop. 2025. PMID: 40852198 Free PMC article. Review.
-
Is reduction necessary in overriding metaphyseal distal radius fractures in children under 11 years: a systematic review and meta-analysis of comparative studies.Eur J Orthop Surg Traumatol. 2024 Jul;34(5):2225-2234. doi: 10.1007/s00590-024-03936-4. Epub 2024 Apr 9. Eur J Orthop Surg Traumatol. 2024. PMID: 38594456
-
Risk stratification for failure of conservative treatment in a cohort of 270 diametaphyseal radius fractures.Arch Orthop Trauma Surg. 2025 May 30;145(1):325. doi: 10.1007/s00402-025-05929-2. Arch Orthop Trauma Surg. 2025. PMID: 40445391 Free PMC article.
-
Therapeutic approaches of diametaphyseal radius fractures in children.Arch Orthop Trauma Surg. 2024 Mar;144(3):1179-1188. doi: 10.1007/s00402-023-05118-z. Epub 2024 Jan 17. Arch Orthop Trauma Surg. 2024. PMID: 38231205
References
-
- Marzi I. Kindertraumatologie. 3rd ed. Springer; Berlin/Heidelberg, Germany: 2016. p. 570.
LinkOut - more resources
Full Text Sources
