

The Dilemma of HSV-1 Oncolytic Virus Delivery: The Method Choice and Hurdles
- PMID: 36835091
- PMCID: PMC9962028
- DOI: 10.3390/ijms24043681
The Dilemma of HSV-1 Oncolytic Virus Delivery: The Method Choice and Hurdles
Abstract
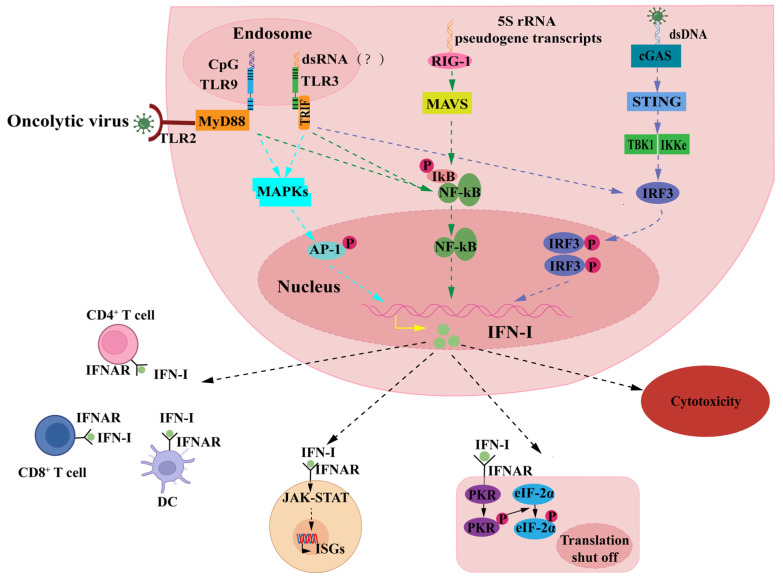
Oncolytic viruses (OVs) have emerged as effective gene therapy and immunotherapy drugs. As an important gene delivery platform, the integration of exogenous genes into OVs has become a novel path for the advancement of OV therapy, while the herpes simplex virus type 1 (HSV-1) is the most commonly used. However, the current mode of administration of HSV-1 oncolytic virus is mainly based on the tumor in situ injection, which limits the application of such OV drugs to a certain extent. Intravenous administration offers a solution to the systemic distribution of OV drugs but is ambiguous in terms of efficacy and safety. The main reason is the synergistic role of innate and adaptive immunity of the immune system in the response against the HSV-1 oncolytic virus, which is rapidly cleared by the body's immune system before it reaches the tumor, a process that is accompanied by side effects. This article reviews different administration methods of HSV-1 oncolytic virus in the process of tumor treatment, especially the research progress in intravenous administration. It also discusses immune constraints and solutions of intravenous administration with the intent to provide new insights into HSV-1 delivery for OV therapy.
Keywords: HSV-1 oncolytic virus therapy; cancer immunotherapy; herpes simplex virus type 1; intravenous injection; mode of administration; oncolytic virus.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Forsyth P., Roldan G., George D., Wallace C., Palmer C.A., Morris D., Cairncross G., Matthews M.V., Markert J., Gillespie Y., et al. A phase I trial of intratumoral administration of reovirus in patients with histologically confirmed recurrent malignant gliomas. Mol. Ther. 2008;16:627–632. doi: 10.1038/sj.mt.6300403. - DOI - PubMed
-
- Patel M.R., Jacobson B.A., Ji Y., Hebbel R.P., Kratzke R.A. Blood Outgrowth Endothelial Cells as a Cellular Carrier for Oncolytic Vesicular Stomatitis Virus Expressing Interferon-beta in Preclinical Models of Non-Small Cell Lung Cancer. Transl. Oncol. 2020;13:100782. doi: 10.1016/j.tranon.2020.100782. - DOI - PMC - PubMed
-
- Monge B M.C., Xie C., Steinberg S.M., Fioraventi S., Walker M., Mabry-Hrones D., Wood B.J., Kleiner D.E., Greten T.F. A phase I/II study of Pexa-Vec oncolytic virus in combination with immune checkpoint inhibition in refractory colorectal cancer. J. Clin. Oncol. 2020;38:117. doi: 10.1200/JCO.2020.38.4_suppl.117. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
