

Novel Molecular Mechanisms Involved in the Medical Treatment of Pulmonary Arterial Hypertension
- PMID: 36835558
- PMCID: PMC9965798
- DOI: 10.3390/ijms24044147
Novel Molecular Mechanisms Involved in the Medical Treatment of Pulmonary Arterial Hypertension
Abstract
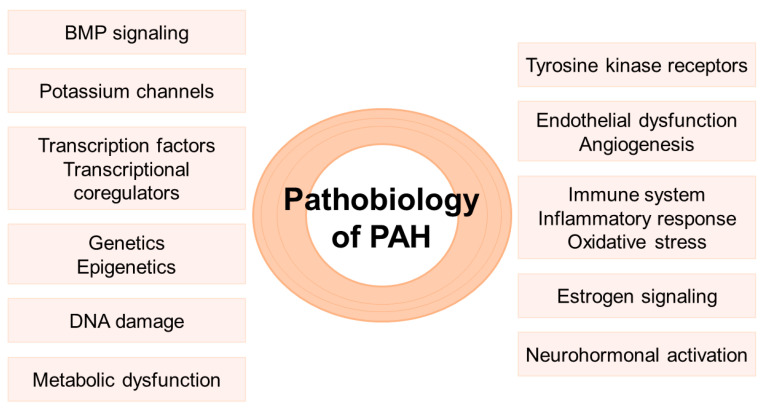
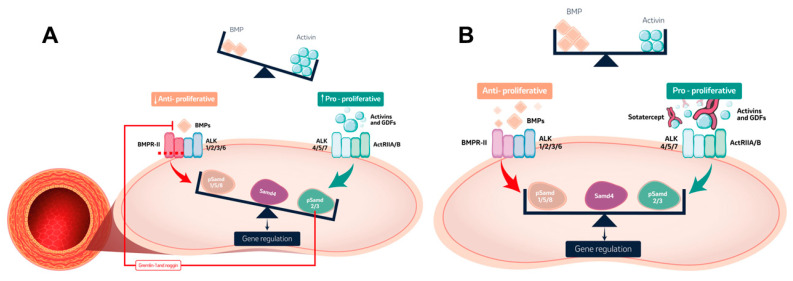
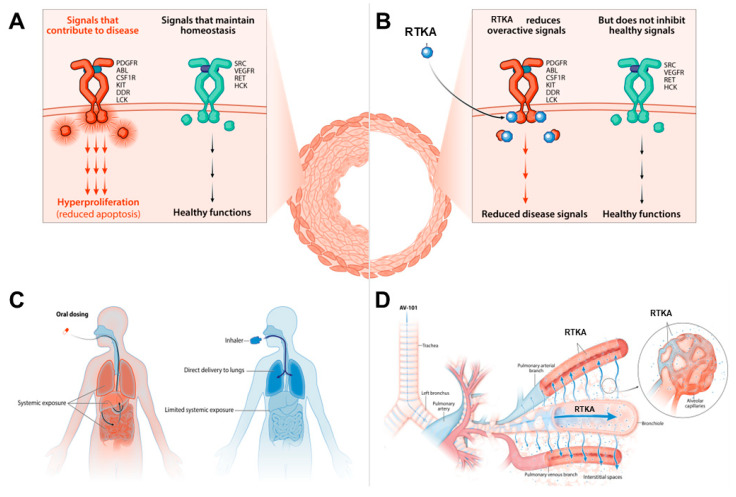
Pulmonary arterial hypertension (PAH) is a severe condition with a high mortality rate despite advances in diagnostic and therapeutic strategies. In recent years, significant scientific progress has been made in the understanding of the underlying pathobiological mechanisms. Since current available treatments mainly target pulmonary vasodilation, but lack an effect on the pathological changes that develop in the pulmonary vasculature, there is need to develop novel therapeutic compounds aimed at antagonizing the pulmonary vascular remodeling. This review presents the main molecular mechanisms involved in the pathobiology of PAH, discusses the new molecular compounds currently being developed for the medical treatment of PAH and assesses their potential future role in the therapeutic algorithms of PAH.
Keywords: BMP signaling; endothelial dysfunction; epigenetics; inflammation; mitochondrial dysfunction; pulmonary arterial hypertension; tyrosine kinase receptor; vascular remodeling.
Conflict of interest statement
P.E-S. has received research grants from Janssen; a speaker honorarium from MSD, Janssen, Ferrer, and AOP; and has participated on a data safety monitoring board and advisory board from MSD, Janssen, Gossamer Bio, AOP, and Ferrer. I.M.d.M. has received a speaker honorarium from Janssen. A.C-U. has received a speaker honorarium from MSD and Janssen; and has participated on a data safety monitoring board and advisory board from Janssen and Gossamer Bio.
Figures
Similar articles
-
Immune Cells in Pulmonary Arterial Hypertension.Heart Lung Circ. 2022 Jul;31(7):934-943. doi: 10.1016/j.hlc.2022.02.007. Epub 2022 Mar 28. Heart Lung Circ. 2022. PMID: 35361533 Review.
-
An emerging strategy for targeted therapy of pulmonary arterial hypertension: Vasodilation plus vascular remodeling inhibition.Drug Discov Today. 2022 May;27(5):1457-1463. doi: 10.1016/j.drudis.2022.01.011. Epub 2022 Jan 29. Drug Discov Today. 2022. PMID: 35104622 Review.
-
Prostaglandin and prostaglandin receptors: present and future promising therapeutic targets for pulmonary arterial hypertension.Respir Res. 2023 Nov 1;24(1):263. doi: 10.1186/s12931-023-02559-3. Respir Res. 2023. PMID: 37915044 Free PMC article. Review.
-
MicroRNAs and their regulators: Potential therapeutic targets in pulmonary arterial hypertension.Vascul Pharmacol. 2023 Dec;153:107216. doi: 10.1016/j.vph.2023.107216. Epub 2023 Sep 10. Vascul Pharmacol. 2023. PMID: 37699495 Review.
-
Egln1Tie2Cre Mice Exhibit Similar Therapeutic Responses to Sildenafil, Ambrisentan, and Treprostinil as Pulmonary Arterial Hypertension (PAH) Patients, Supporting Egln1Tie2Cre Mice as a Useful PAH Model.Int J Mol Sci. 2023 Jan 25;24(3):2391. doi: 10.3390/ijms24032391. Int J Mol Sci. 2023. PMID: 36768713 Free PMC article.
Cited by
-
Advances in Molecular and Translational Medicine.Int J Mol Sci. 2023 Apr 23;24(9):7726. doi: 10.3390/ijms24097726. Int J Mol Sci. 2023. PMID: 37175431 Free PMC article.
-
State of the Art in Pulmonary Arterial Hypertension: Molecular Basis, Imaging Modalities, and Right Heart Failure Treatment.Biomedicines. 2025 Jul 20;13(7):1773. doi: 10.3390/biomedicines13071773. Biomedicines. 2025. PMID: 40722843 Free PMC article. Review.
-
The Relevance of the Endothelium in Cardiopulmonary Disorders.Int J Mol Sci. 2024 Aug 27;25(17):9260. doi: 10.3390/ijms25179260. Int J Mol Sci. 2024. PMID: 39273209 Free PMC article. Review.
-
[Highlights 57th SEPAR Congress].Open Respir Arch. 2024 Sep 5;6(4):100360. doi: 10.1016/j.opresp.2024.100360. eCollection 2024 Oct-Dec. Open Respir Arch. 2024. PMID: 39351171 Free PMC article. Review. Spanish.
-
Haemodynamic spectrum in heritable pulmonary arterial hypertension: a continuum from pre-capillary to combined pulmonary hypertension-case series.Eur Heart J Case Rep. 2025 Feb 26;9(3):ytaf109. doi: 10.1093/ehjcr/ytaf109. eCollection 2025 Mar. Eur Heart J Case Rep. 2025. PMID: 40103798 Free PMC article.
References
-
- Noordegraaf A.V., Chin K., Haddad F., Hassoun P.M., Hemnes A.R., Hopkins S.R., Kawut S.M., Langleben D., Lumens J., Naeije R. Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: An update. Eur. Respir. J. 2019;53:1801900. doi: 10.1183/13993003.01900-2018. - DOI - PMC - PubMed
-
- Humbert M., Kovacs G., Hoeper M.M., Badagliacca R., Berger R.M., Brida M., Carlsen J., Coats A.J., Escribano-Subias P., Ferrari P., et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022;43:3618–3731. doi: 10.1093/eurheartj/ehac237. - DOI - PubMed
-
- Subias P.E., Perez A.A., Olivares C.P., Climent L.G., Cabezudo J.I.D., Perelló M.F. Recent advances in the management of pulmonary arterial hypertension: Lessons from the upfront combination of ambrisentan and tadalafil. Expert Rev. Respir. Med. 2021;15:493–504. doi: 10.1080/17476348.2021.1878027. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
