

Placental Mitochondrial Function and Dysfunction in Preeclampsia
- PMID: 36835587
- PMCID: PMC9963167
- DOI: 10.3390/ijms24044177
Placental Mitochondrial Function and Dysfunction in Preeclampsia
Abstract
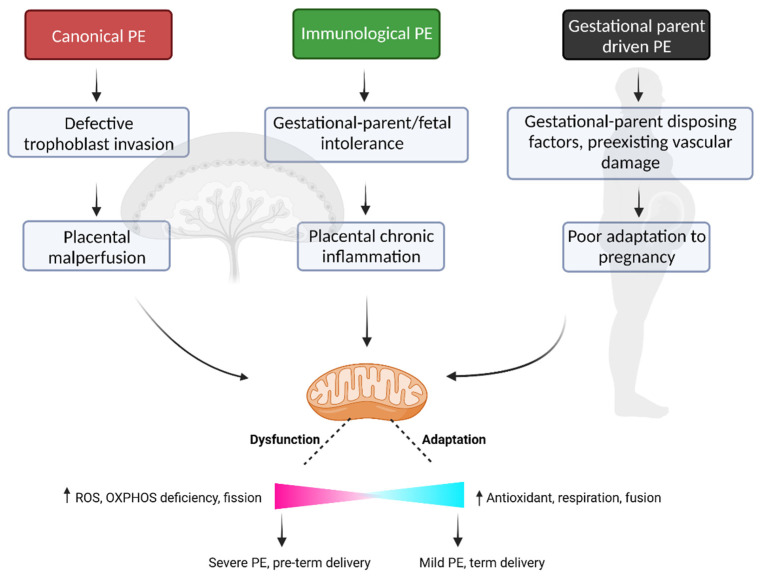
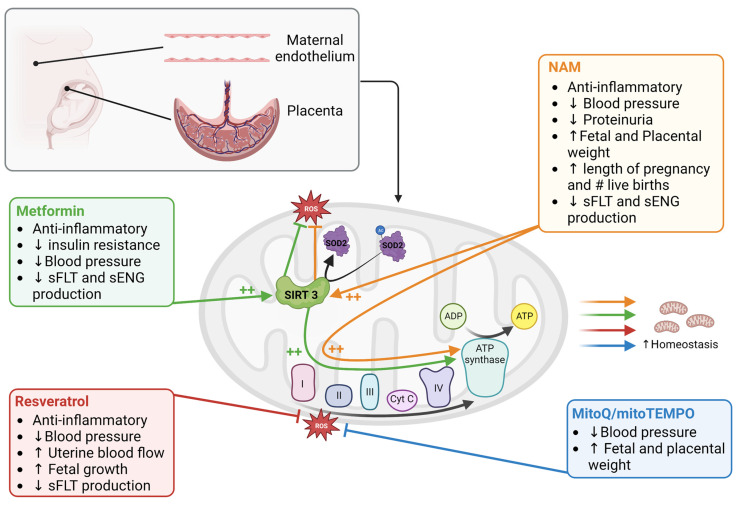
The placenta is a vital organ of pregnancy, regulating adaptation to pregnancy, gestational parent/fetal exchange, and ultimately, fetal development and growth. Not surprisingly, in cases of placental dysfunction-where aspects of placental development or function become compromised-adverse pregnancy outcomes can result. One common placenta-mediated disorder of pregnancy is preeclampsia (PE), a hypertensive disorder of pregnancy with a highly heterogeneous clinical presentation. The wide array of clinical characteristics observed in pregnant individuals and neonates of a PE pregnancy are likely the result of distinct forms of placental pathology underlying the PE diagnosis, explaining why no one common intervention has proven effective in the prevention or treatment of PE. The historical paradigm of placental pathology in PE highlights an important role for utero-placental malperfusion, placental hypoxia and oxidative stress, and a critical role for placental mitochondrial dysfunction in the pathogenesis and progression of the disease. In the current review, the evidence of placental mitochondrial dysfunction in the context of PE will be summarized, highlighting how altered mitochondrial function may be a common feature across distinct PE subtypes. Further, advances in this field of study and therapeutic targeting of mitochondria as a promising intervention for PE will be discussed.
Keywords: disease subclasses; hypertension; mitochondria; placenta; preeclampsia; pregnancy; reactive oxygen species; therapies.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Griffiths S.K., Campbell J.P. Placental structure, function and drug transfer. Contin. Educ. Anaesth. Crit. Care Pain. 2014;15:84–89. doi: 10.1093/bjaceaccp/mku013. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
