

Is There a High Risk for GI Bleeding Complications in Patients Undergoing Abdominal Surgery?
- PMID: 36835910
- PMCID: PMC9965273
- DOI: 10.3390/jcm12041374
Is There a High Risk for GI Bleeding Complications in Patients Undergoing Abdominal Surgery?
Abstract
Introduction: Gastrointestinal bleeding (GIB) can cause life-threatening situations. Here, endoscopy is the first-line diagnostic and therapeutic mode in patients with GIB among further therapeutic approaches such as embolization or medical treatment. Although GIB is considered the most common indication for emergency endoscopy in clinical practice, data on GIB in abdominal surgical patients are still scarce.
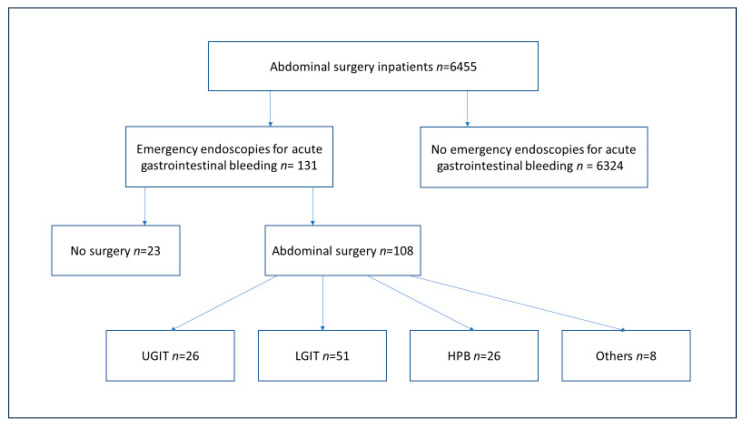
Patients and methods: For the present study, all emergency endoscopies performed on hospitalized abdominal surgical patients over a 2-year period (1 July 2017-30 June2019) were retrospectively analyzed. Primary endpoint was 30-day mortality. Secondary endpoints were length of hospital stay, cause of bleeding, and therapeutic success of endoscopic intervention.
Results: During the study period, bleeding events with an indication for emergency endoscopy occurred in 2.0% (129/6455) of all surgical inhouse patients, of whom 83.7% (n = 108) underwent a surgical procedure. In relation to the total number of respective surgical procedures during the study period, the bleeding incidence was 8.9% after hepatobiliary surgery, 7.7% after resections in the upper gastrointestinal tract, and 1.1% after colonic resections. Signs of active or past bleeding in the anastomosis area were detected in ten patients (6.9%). The overall 30-day mortality was 7.75%.
Conclusions: The incidence of relevant gastrointestinal bleeding events in visceral surgical inpatients was overall rare. However, our data call for critical peri-operative vigilance for bleeding events and underscore the importance of interdisciplinary emergency algorithms.
Keywords: bleeding after GI surgery; endoscopic complication management; postoperative gastrointestinal bleeding.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Relevance of surgery in patients with non-variceal upper gastrointestinal bleeding.Langenbecks Arch Surg. 2017 May;402(3):509-519. doi: 10.1007/s00423-017-1552-2. Epub 2017 Jan 14. Langenbecks Arch Surg. 2017. PMID: 28091770
-
Endoscopic Algorithm for Management of Gastrointestinal Bleeding in Patients With Continuous Flow LVADs: A Prospective Validation Study.J Card Fail. 2020 Apr;26(4):324-332. doi: 10.1016/j.cardfail.2019.11.027. Epub 2019 Dec 1. J Card Fail. 2020. PMID: 31794863 Free PMC article.
-
Clinical Predictors for Repeat Hospitalizations in Left Ventricular Assist Device (LVAD) Patients With Gastrointestinal Bleeding.Gastroenterology Res. 2018 Apr;11(2):100-105. doi: 10.14740/gr972w. Epub 2018 Apr 7. Gastroenterology Res. 2018. PMID: 29707076 Free PMC article.
-
Transcatheter arterial embolization versus surgery for refractory non-variceal upper gastrointestinal bleeding: a meta-analysis.World J Emerg Surg. 2019 Feb 1;14:3. doi: 10.1186/s13017-019-0223-8. eCollection 2019. World J Emerg Surg. 2019. PMID: 30733822 Free PMC article.
-
Systematic reviews of the clinical effectiveness and cost-effectiveness of proton pump inhibitors in acute upper gastrointestinal bleeding.Health Technol Assess. 2007 Dec;11(51):iii-iv, 1-164. doi: 10.3310/hta11510. Health Technol Assess. 2007. PMID: 18021578 Review.
Cited by
-
Surgery and Reason: The End of History and the Last Surgeon.J Clin Med. 2023 Sep 1;12(17):5708. doi: 10.3390/jcm12175708. J Clin Med. 2023. PMID: 37685775 Free PMC article.
References
-
- Gotz M., Anders M., Biecker E., Bojarski C., Braun G., Brechmann T., Dechene A., Dollinger M., Gawaz M., Kiesslich R., et al. s2k guideline gastrointestinal bleeding—Guideline of the german society of gastroenterology dgvs. Z. Gastroenterol. 2017;55:883–936. doi: 10.1055/s-0043-116856. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
