

Effects of Individualised High Positive End-Expiratory Pressure and Crystalloid Administration on Postoperative Pulmonary Function in Patients Undergoing Robotic-Assisted Radical Prostatectomy: A Prospective Randomised Single-Blinded Pilot Study
- PMID: 36835995
- PMCID: PMC9960679
- DOI: 10.3390/jcm12041460
Effects of Individualised High Positive End-Expiratory Pressure and Crystalloid Administration on Postoperative Pulmonary Function in Patients Undergoing Robotic-Assisted Radical Prostatectomy: A Prospective Randomised Single-Blinded Pilot Study
Abstract
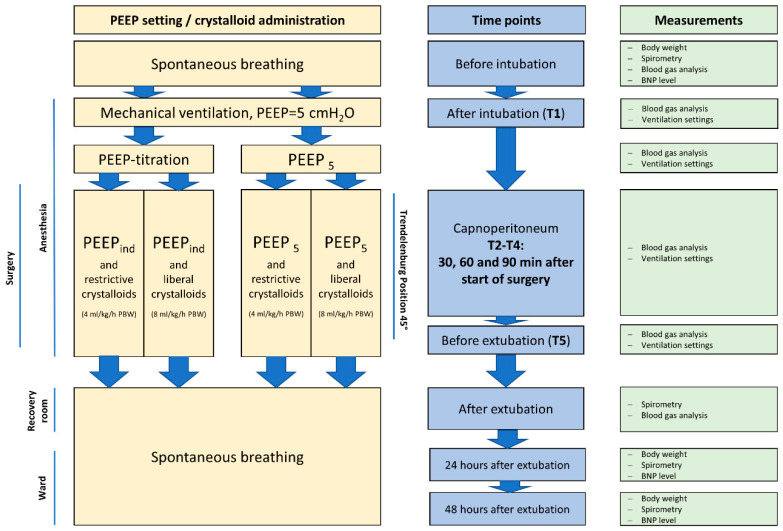
Objectives: Robotic-assisted laparoscopic prostatectomy (RALP) is typically conducted in steep Trendelenburg position (STP). The aim of the study was to evaluate whether crystalloid administration and individual management of positive end-expiratory pressure (PEEP) improve peri- and post-operative pulmonary function in patients undergoing RALP.
Design: Prospective randomised single-centre single-blinded explorative study.
Setting: Patients were either allocated to a standard PEEP (5 cmH2O) group or an individualised high PEEP group. Furthermore, each group was divided into a liberal and a restrictive crystalloid group (8 vs. 4 mL/kg/h predicted body weight). Individualised PEEP levels were determined by means of preoperative recruitment manoeuvre and PEEP titration in STP.
Participants: Informed consent was obtained from 98 patients scheduled for elective RALP.
Interventions: The following intraoperative parameters were analysed in each of the four study groups: ventilation setting (peak inspiratory pressure [PIP], plateau pressure, driving pressure [Pdriv], lung compliance [LC] and mechanical power [MP]) and postoperative pulmonary function (bed-side spirometry). The spirometric parameters Tiffeneau index (FEV1/FVC ratio) and mean forced expiratory flow (FEF25-75) were measured pre- and post-operatively. Data are shown as mean ± standard deviation (SD), and groups were compared with ANOVA. A p-value of <0.05 was considered significant.
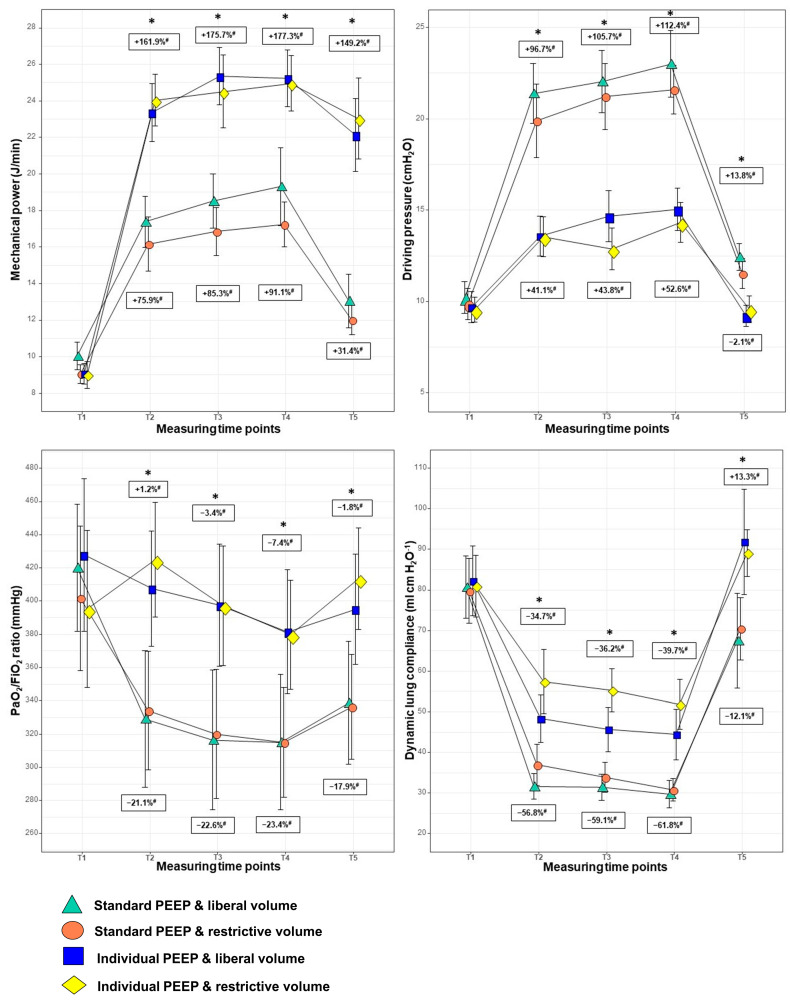
Results: The two individualised high PEEP groups (mean PEEP 15.5 [±1.71 cmH2O]) showed intraoperative significantly higher PIP, plateau pressure and MP levels but significantly decreased Pdriv and increased LC. On the first and second postoperative day, patients with individualised high PEEP levels had a significantly higher mean Tiffeneau index and FEF25-75. Perioperative oxygenation and ventilation and postoperative spirometric parameters were not influenced by restrictive or liberal crystalloid infusion in either of the two respective PEEP groups.
Conclusions: Individualised high PEEP levels (≥14 cmH2O) during RALP improved intraoperative blood oxygenation and resulted in more lung-protective ventilation. Furthermore, postoperative pulmonary function was improved for up to 48 h after surgery in the sum of the two individualised high PEEP groups. Restrictive crystalloid infusion during RALP seemed to have no effect on peri- and post-operative oxygenation and pulmonary function.
Keywords: fluid management; individual PEEP; pulmonary function; robotic-assisted laparoscopic prostatectomy; steep Trendelenburg position.
Conflict of interest statement
All authors declare no competing interests in relation to this paper.
Figures
References
-
- Tewari A., Sooriakumaran P., Bloch D.A., Seshadri-Kreaden U., Hebert A.E., Wiklund P. Positive Surgical Margin and Perioperative Complication Rates of Primary Surgical Treatments for Prostate Cancer: A Systematic Review and Meta-Analysis Comparing Retropubic, Laparoscopic, and Robotic Prostatectomy. Eur. Urol. 2012;62:1–15. doi: 10.1016/j.eururo.2012.02.029. - DOI - PubMed
-
- Novara G., Ficarra V., Rosen R.C., Artibani W., Costello A., Eastham J.A., Graefen M., Guazzoni G., Shariat S.F., Stolzenburg J., et al. Systematic review and meta-analysis of perioperative outcomes and complications after robot-assisted radical prostatectomy. Eur. Urol. 2012;62:431–452. doi: 10.1016/j.eururo.2012.05.044. - DOI - PubMed
-
- Ficarra V., Novara G., Artibani W., Cestari A., Galfano A., Graefen M., Guazzoni G., Guillonneau B., Menon M., Montorsi F., et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: A systematic review and cumulative analysis of comparative studies. Eur. Urol. 2009;55:1037–1063. doi: 10.1016/j.eururo.2009.01.036. - DOI - PubMed
-
- Gainsburg D.M. Anesthetic concerns for robotic-assisted laparoscopic radical prostatectomy. Minerva Anestesiol. 2012;78:596–604. - PubMed
LinkOut - more resources
Full Text Sources
