

Invasive Pulmonary Aspergillosis
- PMID: 36836246
- PMCID: PMC9962768
- DOI: 10.3390/jof9020131
Invasive Pulmonary Aspergillosis
Abstract
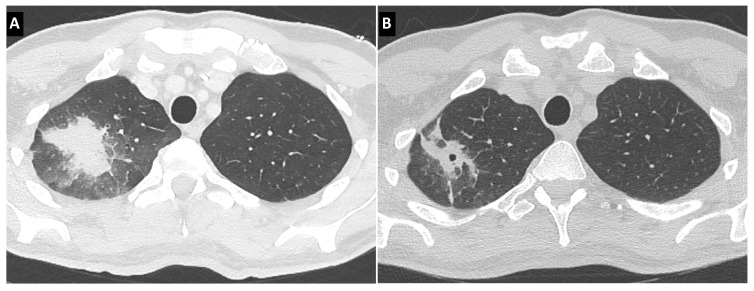
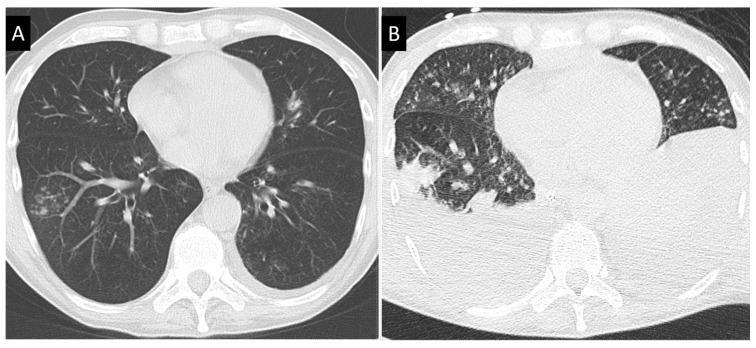
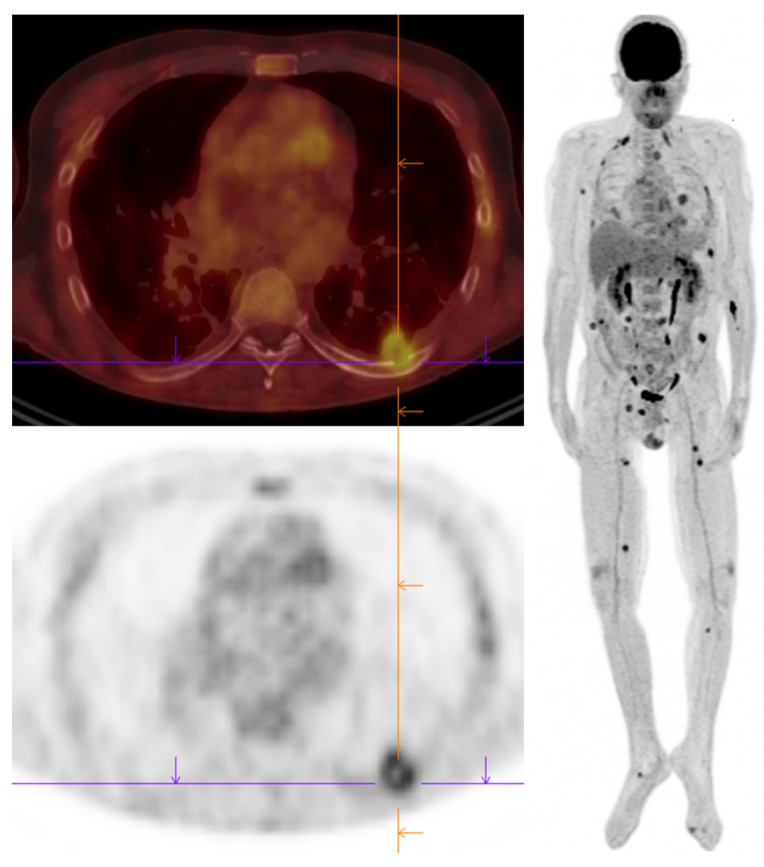
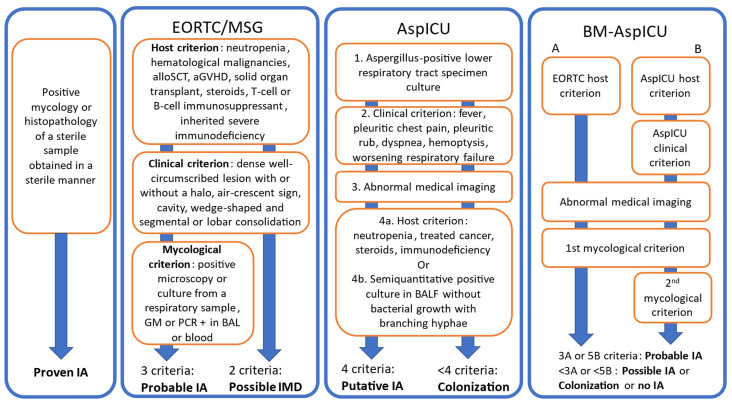
Invasive pulmonary aspergillosis is growing in incidence, as patients at risk are growing in diversity. Outside the classical context of neutropenia, new risk factors are emerging or newly identified, such as new anticancer drugs, viral pneumonias and hepatic dysfunctions. Clinical signs remain unspecific in these populations and the diagnostic work-up has considerably expanded. Computed tomography is key to assess the pulmonary lesions of aspergillosis, whose various features must be acknowledged. Positron-emission tomography can bring additional information for diagnosis and follow-up. The mycological argument for diagnosis is rarely fully conclusive, as biopsy from a sterile site is challenging in most clinical contexts. In patients with a risk and suggestive radiological findings, probable invasive aspergillosis is diagnosed through blood and bronchoalveolar lavage fluid samples by detecting galactomannan or DNA, or by direct microscopy and culture for the latter. Diagnosis is considered possible with mold infection in lack of mycological criterion. Nevertheless, the therapeutic decision should not be hindered by these research-oriented categories, that have been completed by better adapted ones in specific settings. Survival has been improved over the past decades with the development of relevant antifungals, including lipid formulations of amphotericin B and new azoles. New antifungals, including first-in-class molecules, are awaited.
Keywords: galactomannan; hematopoietic stem cell transplantation; isavuconazole; leukemia; liposomal amphotericin B; neutropenia; posaconazole; review; solid organ transplantation; voriconazole.
Conflict of interest statement
Ledoux reports personal fees from Gilead, personal fees from Pfizer, personal fees from Abbvie, personal fees from Novartis, outside the submitted work. Herbrecht reports personal fees from Gilead and Mundipharma and research grant from Gilead.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
