

Pulmonary Histoplasmosis: A Clinical Update
- PMID: 36836350
- PMCID: PMC9964986
- DOI: 10.3390/jof9020236
Pulmonary Histoplasmosis: A Clinical Update
Abstract
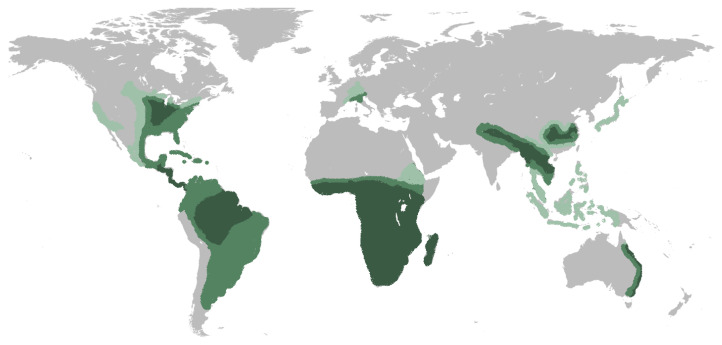
Histoplasma capsulatum, the etiological agent for histoplasmosis, is a dimorphic fungus that grows as a mold in the environment and as a yeast in human tissues. The areas of highest endemicity lie within the Mississippi and Ohio River Valleys of North America and parts of Central and South America. The most common clinical presentations include pulmonary histoplasmosis, which can resemble community-acquired pneumonia, tuberculosis, sarcoidosis, or malignancy; however, certain patients can develop mediastinal involvement or progression to disseminated disease. Understanding the epidemiology, pathology, clinical presentation, and diagnostic testing performance is pivotal for a successful diagnosis. While most immunocompetent patients with mild acute or subacute pulmonary histoplasmosis should receive therapy, all immunocompromised patients and those with chronic pulmonary disease or progressive disseminated disease should also receive therapy. Liposomal amphotericin B is the agent of choice for severe or disseminated disease, and itraconazole is recommended in milder cases or as "step-down" therapy after initial improvement with amphotericin B. In this review, we discuss the current epidemiology, pathology, diagnosis, clinical presentations, and management of pulmonary histoplasmosis.
Keywords: histoplasmosis; pulmonary histoplasmosis.
Conflict of interest statement
The authors declare no conflict of interest.
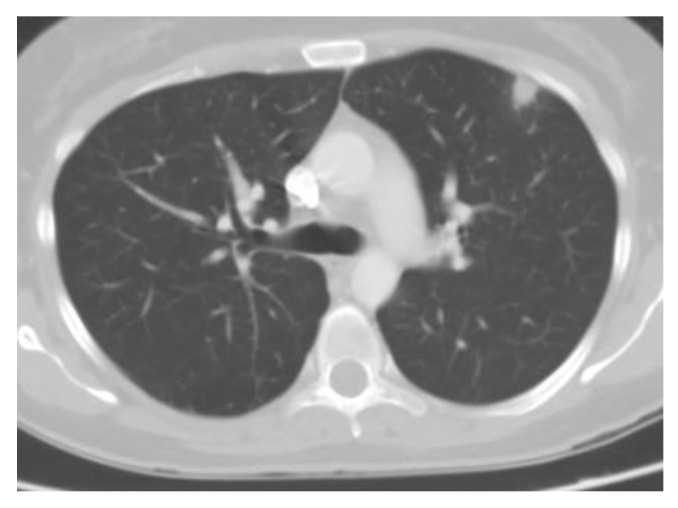
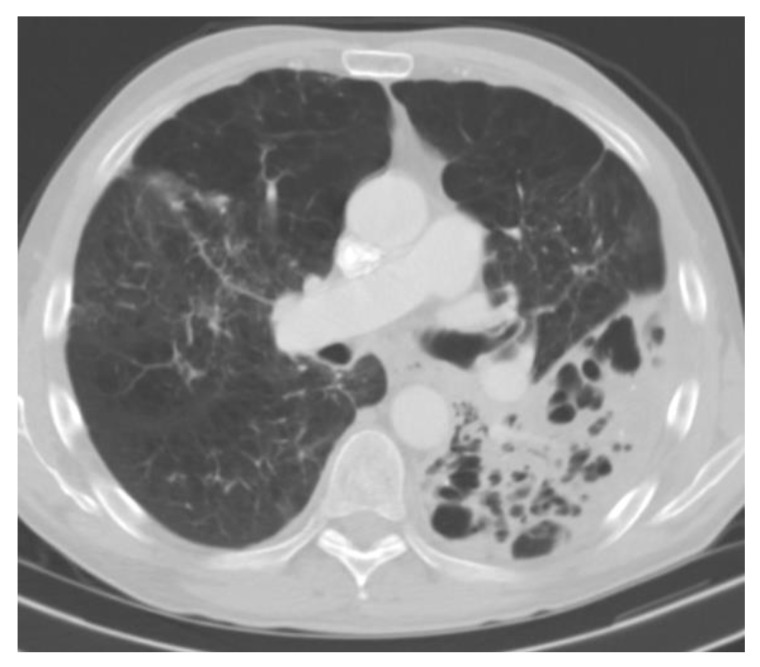
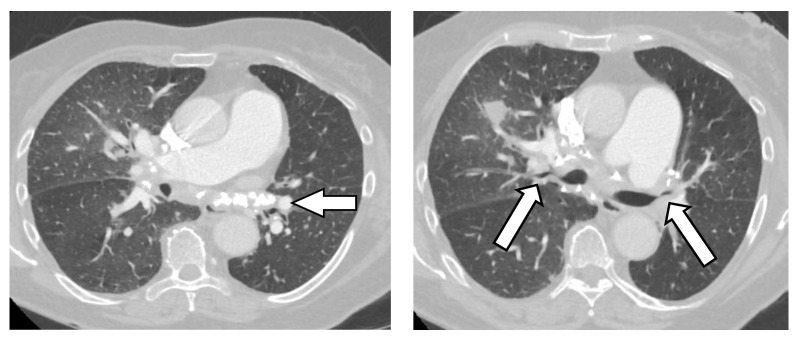
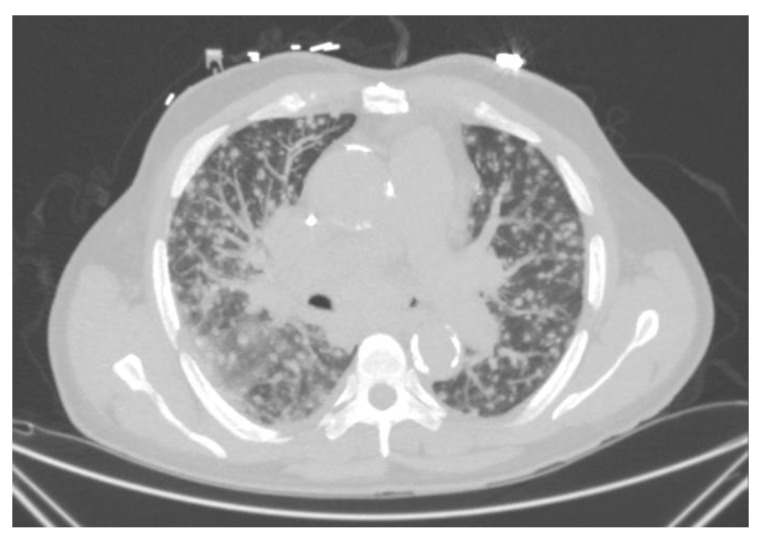
Figures
Similar articles
-
Current Concepts in the Epidemiology, Diagnosis, and Management of Histoplasmosis Syndromes.Semin Respir Crit Care Med. 2020 Feb;41(1):13-30. doi: 10.1055/s-0039-1698429. Epub 2020 Jan 30. Semin Respir Crit Care Med. 2020. PMID: 32000281 Review.
-
Histoplasmosis: Up-to-Date Evidence-Based Approach to Diagnosis and Management.Semin Respir Crit Care Med. 2015 Oct;36(5):729-45. doi: 10.1055/s-0035-1562899. Epub 2015 Sep 23. Semin Respir Crit Care Med. 2015. PMID: 26398539 Review.
-
Treatment of histoplasmosis.Semin Respir Infect. 2001 Jun;16(2):141-8. doi: 10.1053/srin.2001.24244. Semin Respir Infect. 2001. PMID: 11521246 Review.
-
Disseminated Histoplasmosis: A Rare Cause of Pancytopenia in an Immunocompromised Patient.Cureus. 2022 Jun 15;14(6):e25966. doi: 10.7759/cureus.25966. eCollection 2022 Jun. Cureus. 2022. PMID: 35720778 Free PMC article.
-
Clinical Perspectives in the Diagnosis and Management of Histoplasmosis.Clin Chest Med. 2017 Sep;38(3):403-415. doi: 10.1016/j.ccm.2017.04.004. Epub 2017 May 17. Clin Chest Med. 2017. PMID: 28797485 Review.
Cited by
-
Progressive Encephalopathy With New Pulmonary Opacities in an Immunocompromised Host.CHEST Crit Care. 2024 Jun;2(2):100064. doi: 10.1016/j.chstcc.2024.100064. Epub 2024 Mar 11. CHEST Crit Care. 2024. PMID: 38938509 Free PMC article.
-
Histoplasma seropositivity and environmental risk factors for exposure in a general population in Upper River Region, The Gambia: A cross-sectional study.One Health. 2024 Mar 27;18:100717. doi: 10.1016/j.onehlt.2024.100717. eCollection 2024 Jun. One Health. 2024. PMID: 38576541 Free PMC article.
-
Unmasking Histoplasmosis: A Diagnostic Challenge of Pediatric Febrile Neutropenia in an Immunocompromised Patient.Cureus. 2025 Jul 17;17(7):e88208. doi: 10.7759/cureus.88208. eCollection 2025 Jul. Cureus. 2025. PMID: 40687412 Free PMC article.
-
Pulmonary cryptococcosis with headache as the first presentation: A case report.Open Life Sci. 2025 Aug 12;20(1):20251119. doi: 10.1515/biol-2025-1119. eCollection 2025. Open Life Sci. 2025. PMID: 40822967 Free PMC article.
-
Disseminated Histoplasmosis Diagnosed in an Immunocompetent Patient from a Non-Endemic Area: Neglected or Emerging Disease?Diagnostics (Basel). 2024 Oct 5;14(19):2219. doi: 10.3390/diagnostics14192219. Diagnostics (Basel). 2024. PMID: 39410623 Free PMC article.
References
-
- Edwards L.B., Acquaviva F.A., Livesay V.T., Cross F.W., Palmer C.E. An atlas of sensitivity to tuberculin, PPD-B, and histoplasmin in the United States. Am. Rev. Respir. Dis. 1969;99((Suppl. 1)):132. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
