

Myopia Control with Low-Dose Atropine in European Children: Six-Month Results from a Randomized, Double-Masked, Placebo-Controlled, Multicenter Study
- PMID: 36836559
- PMCID: PMC9960354
- DOI: 10.3390/jpm13020325
Myopia Control with Low-Dose Atropine in European Children: Six-Month Results from a Randomized, Double-Masked, Placebo-Controlled, Multicenter Study
Abstract
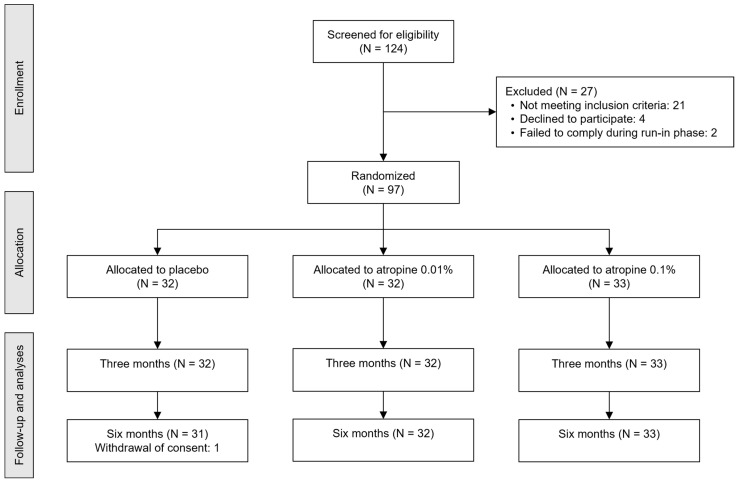
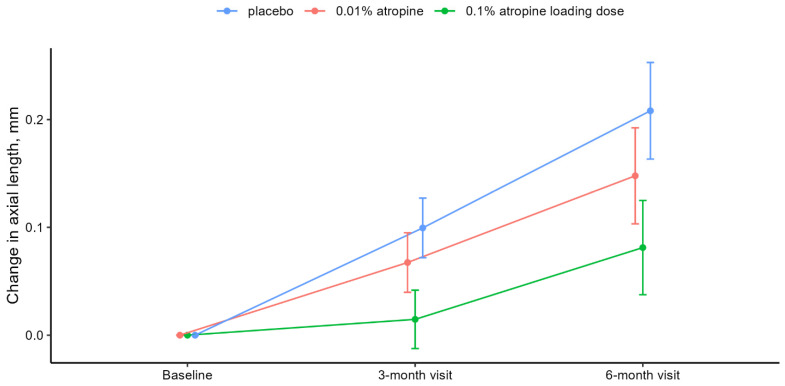
The effect and safety of low-dose atropine in myopia control have not been studied in randomized, placebo-controlled trials outside Asia. We investigated the efficacy and safety of 0.1% atropine loading dose and 0.01% atropine compared with a placebo in a European population. Investigator-initiated, randomized, double-masked, placebo-controlled, equal-allocation, multicenter study comparing 0.1% atropine loading dose (six months) followed by 0.01% atropine (18 months), 0.01% atropine (24 months), and placebo (24 months). Participants were monitored for a 12-months washout period. Outcome measures were axial length (AL), cycloplegic spherical equivalent (SE), photopic and mesopic pupil size, accommodation amplitude, visual acuity, intraocular pressure (IOP), and adverse reactions and events. We randomized 97 participants (mean [standard deviation] age, 9.4 [1.7] years; 55 girls (57%) and 42 boys (43%)). After six months, AL was 0.13 mm shorter (95% confidence interval [CI], -0.18 to -0.07 [adjusted p < 0.001]) with 0.1% atropine loading dose and 0.06 mm shorter (95% CI, -0.11 to -0.01 [adjusted p = 0.06]) with 0.01% atropine than in the placebo group. We observed similar dose-dependent changes in SE, pupil size, accommodation amplitude, and adverse reactions. No significant differences in visual acuity or IOP were found between groups, and no serious adverse reactions were reported. We found a dose-dependent effect of low-dose atropine in European children without adverse reactions requiring photochromatic or progressive spectacles. Our results are comparable to those observed in East Asia, indicating that results on myopia control with low-dose atropine are generalizable across populations with different racial backgrounds.
Keywords: axial length; low-dose atropine; myopia; myopia control; spherical equivalent.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Williams K.M., Verhoeven V., Cumberland P.M., Bertelsen G., Wolfram C., Buitendijk G.H.S., Hofman A., Van Duijn C.M., Vingerling J.R., Kuijpers R.W.A.M., et al. Prevalence of refractive error in Europe: The European Eye Epidemiology (E(3)) Consortium. Eur. J. Epidemiol. 2015;30:305–315. doi: 10.1007/s10654-015-0010-0. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
