

A Meta-Analysis of Sampled Maximal Aerobic Capacity Data for Boys Aged 11 Years Old or Less Obtained by Cycle Ergometry
- PMID: 36836634
- PMCID: PMC9967809
- DOI: 10.3390/life13020276
A Meta-Analysis of Sampled Maximal Aerobic Capacity Data for Boys Aged 11 Years Old or Less Obtained by Cycle Ergometry
Abstract
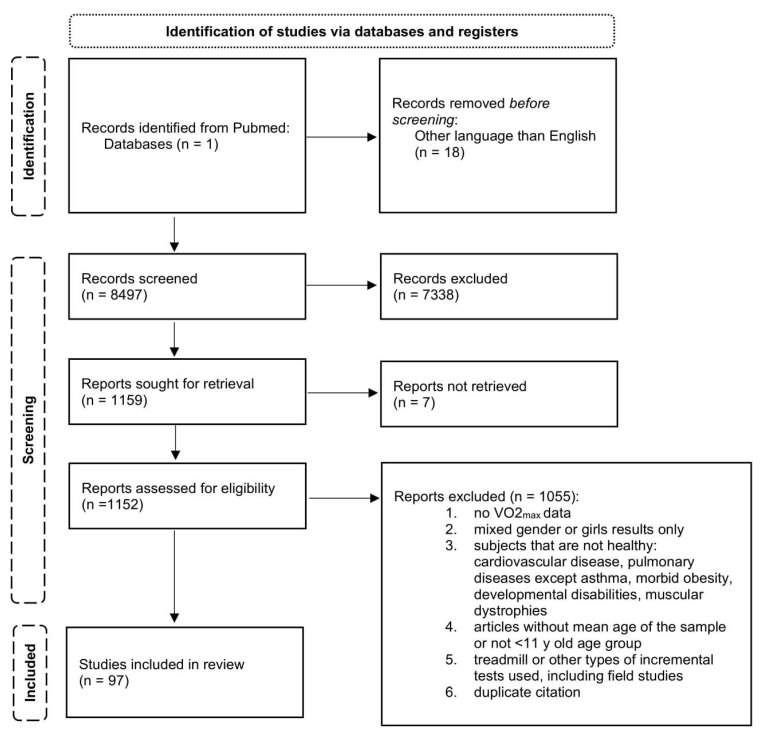
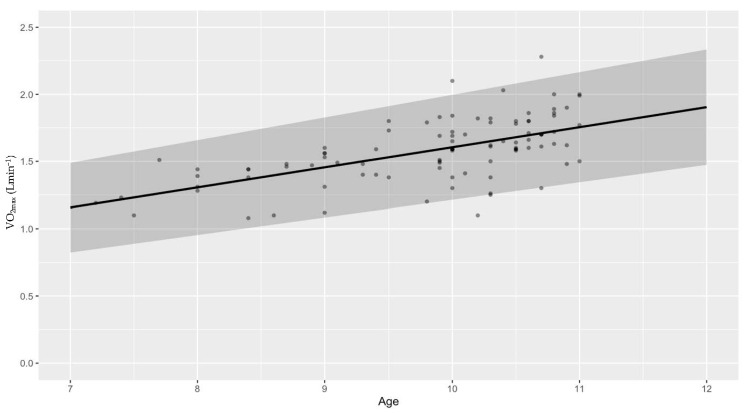
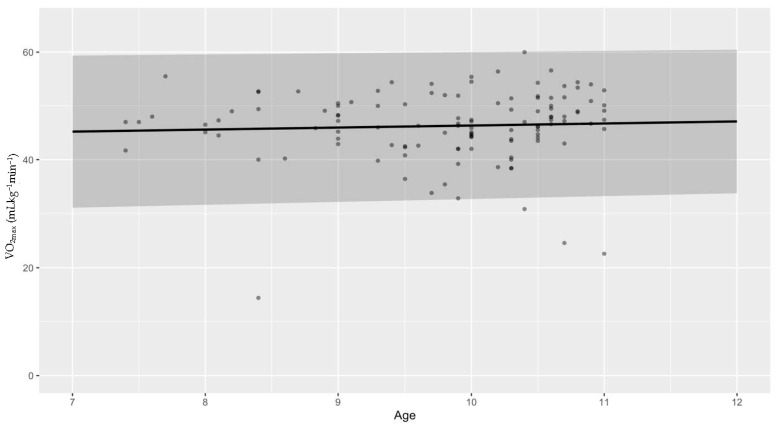
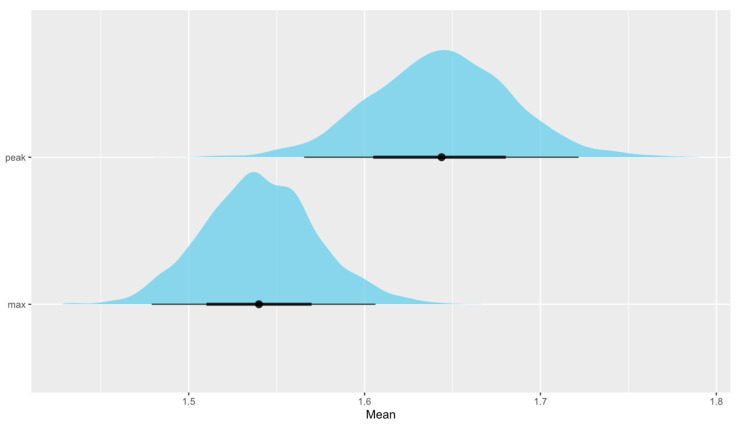
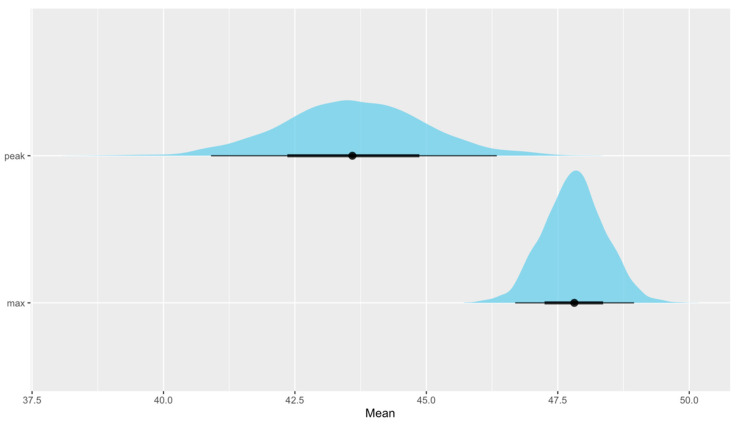
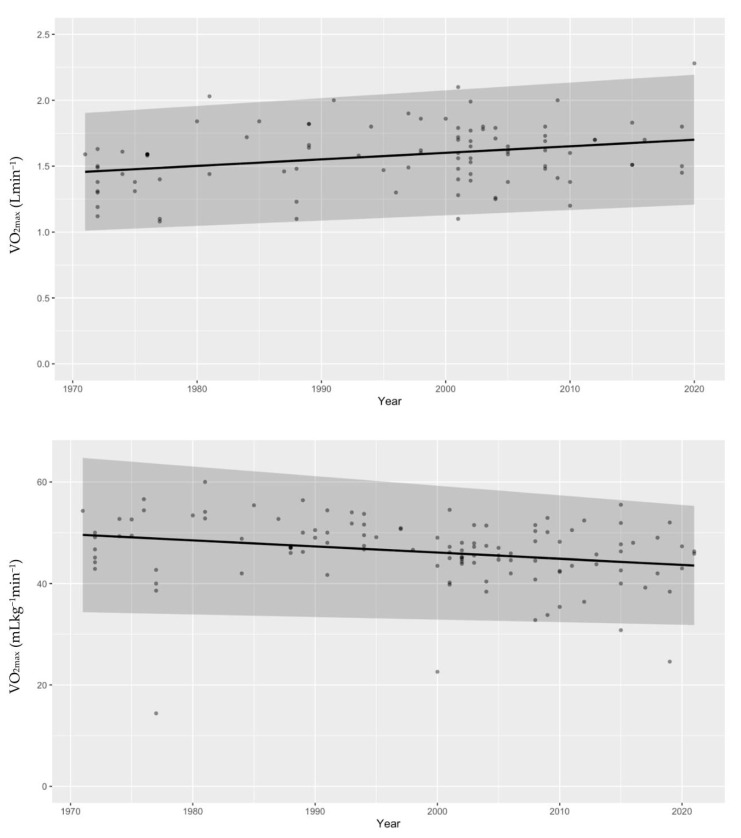
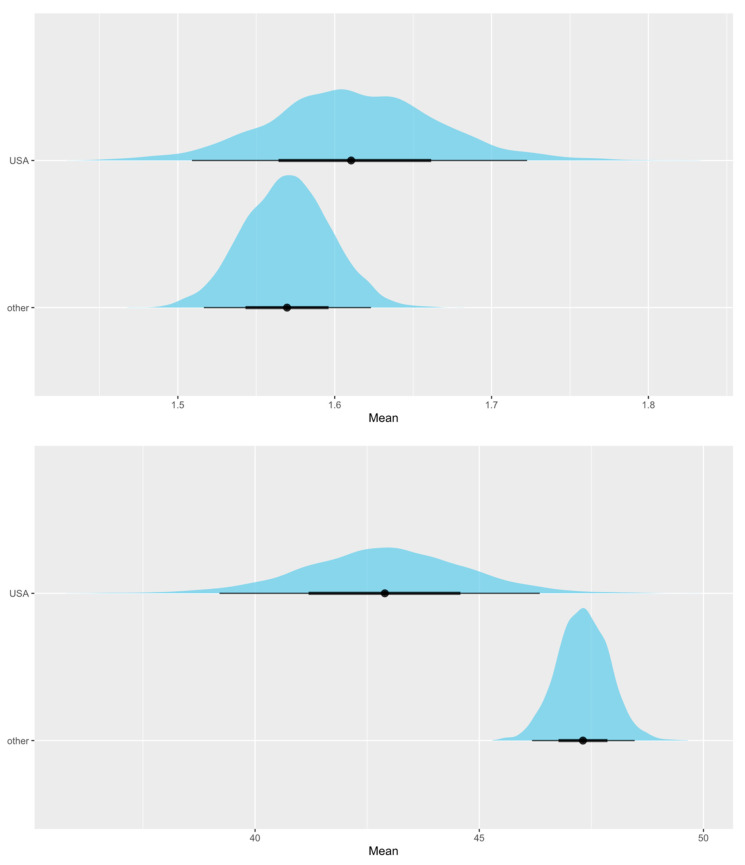
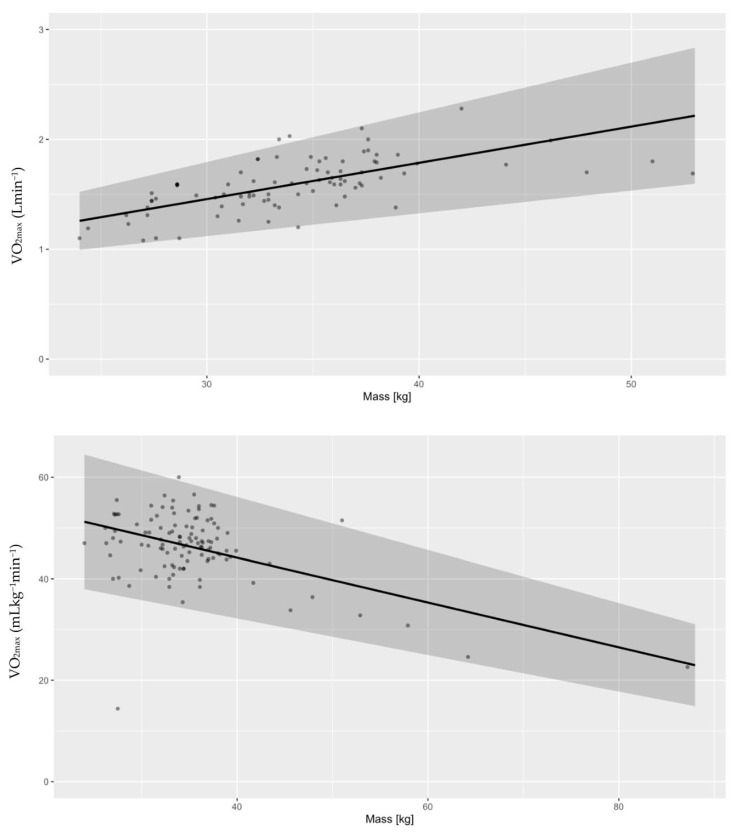
The aim of this study was to develop distributions of VO2max based on measured values that exist in the literature in prepubertal boys using cycle ergometry. PRISMA guidelines were followed in conducting this research. One database was searched for peak and maximal VO2 values in healthy boys with mean age under 11 years old. Data were split into articles reporting absolute and relative VO2max values and analyzed accordingly. Multilevel models grounded in Bayesian principles were used. We investigated associations between VO2max and body mass, year of the study, and country of origin. Differences in "peak" and "maximal" VO2 were assessed. Absolute VO2max (Lmin-1) increases with age (P ~100%) but mean relative VO2max does not change (P ~100%). Absolute VO2max is higher in more recent studies (P = 95.7 ± 0.3%) and mean relative VO2max is lower (P = 99.6 ± 0.1%). Relative VO2max in the USA is lower compared with boys from other countries (P = 98.8 ± 0.2%), but there are no differences in absolute values. Mean aerobic capacity estimates presented as "peak" values are higher than "maximal" values on an absolute basis (P = 97.5 ± 0.3%) but not on a relative basis (P = 99.6 ± 0.1%). Heavier boys have lower cardiorespiratory fitness (P ≈ 100%), and body mass seems to be increasing faster with age in the USA compared with other countries (P = 92.3 ± 0.3%). New reference values for cardiorespiratory fitness are presented for prepubertal boys obtained with cycle ergometry. This is new, as no reference values have been determined so far based on actual measured values in prepubertal boys. Aerobic capacity normalized to body weight does not change with age. Cardiorespiratory fitness in prepubertal boys is declining, which is associated with increasing body mass over the last few decades. Lastly, this study did not find any statistically significant difference in the sample's mean aerobic capacity estimates using the "peak" and "maximum" distinctions identified in the literature.
Keywords: aerobic fitness; boys; children; cycle ergometry; maximal oxygen consumption.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Balady G.J., Arena R., Sietsema K., Myers J., Coke L., Fletcher G.F., Forman D., Franklin B., Guazzi M., Gulati M., et al. Clinician’s Guide to Cardiopulmonary Exercise Testing in Adults: A Scientific Statement from the American Heart Association. Circulation. 2010;122:191–225. doi: 10.1161/CIR.0b013e3181e52e69. - DOI - PubMed
-
- Palange P., Laveneziana P., Neder J.A., Ward S.A. In: Clinical Exercise Testing. Palange P., Laveneziana P., Neder J.A., Ward S.A., editors. European Respiratory Society; Sheffield, UK: 2018.
Publication types
LinkOut - more resources
Full Text Sources
