

Current Views on Infective Endocarditis: Changing Epidemiology, Improving Diagnostic Tools and Centering the Patient for Up-to-Date Management
- PMID: 36836734
- PMCID: PMC9965398
- DOI: 10.3390/life13020377
Current Views on Infective Endocarditis: Changing Epidemiology, Improving Diagnostic Tools and Centering the Patient for Up-to-Date Management
Abstract
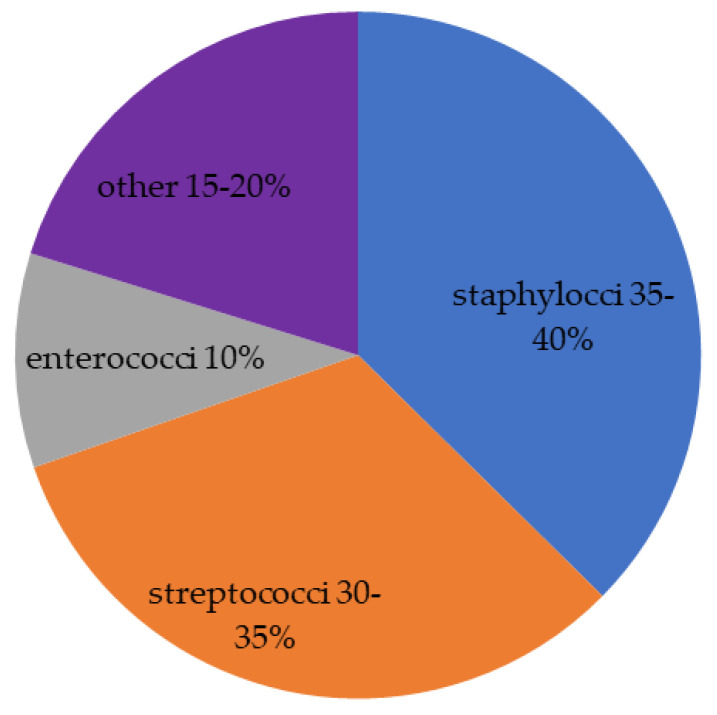
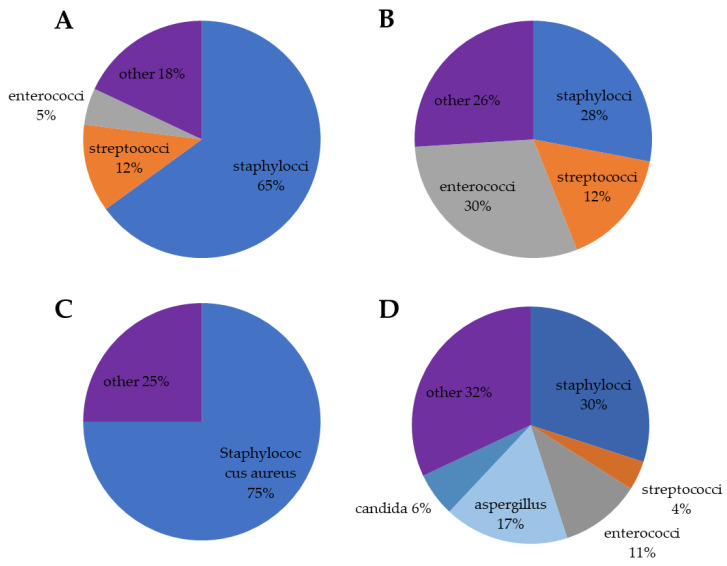
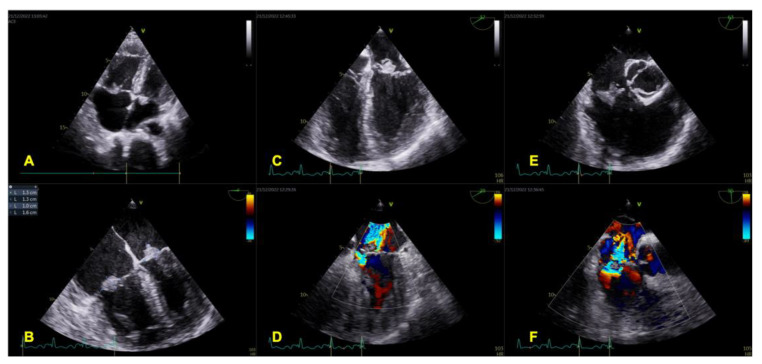
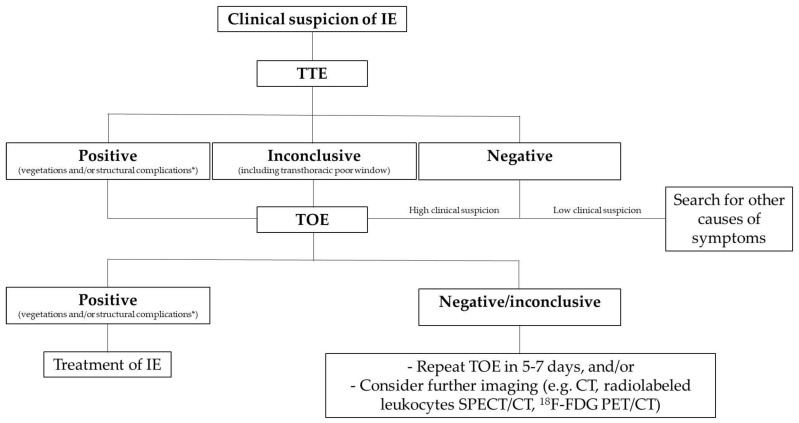
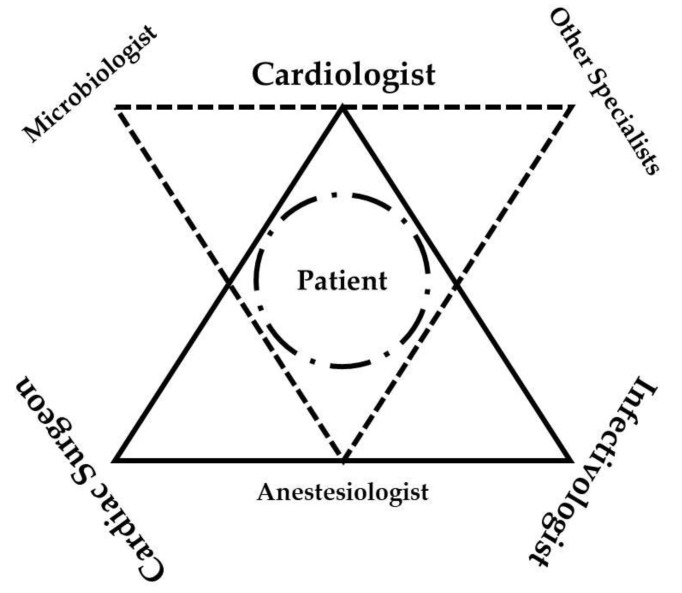
Infective endocarditis (IE) is a rare but potentially life-threatening disease, sometimes with longstanding sequels among surviving patients. The population at high risk of IE is represented by patients with underlying structural heart disease and/or intravascular prosthetic material. Taking into account the increasing number of intravascular and intracardiac procedures associated with device implantation, the number of patients at risk is growing too. If bacteremia develops, infected vegetation on the native/prosthetic valve or any intracardiac/intravascular device may occur as the final result of invading microorganisms/host immune system interaction. In the case of IE suspicion, all efforts must be focused on the diagnosis as IE can spread to almost any organ in the body. Unfortunately, the diagnosis of IE might be difficult and require a combination of clinical examination, microbiological assessment and echocardiographic evaluation. There is a need of novel microbiological and imaging techniques, especially in cases of blood culture-negative. In the last few years, the management of IE has changed. A multidisciplinary care team, including experts in infectious diseases, cardiology and cardiac surgery, namely, the Endocarditis Team, is highly recommended by the current guidelines.
Keywords: antibiotics; imaging technique; infection; multidisciplinary team.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Cimmino G., Ciccarelli G., Golino M., D’Amico C., Golino P. A Fatal Case of Endocarditis on CoreValve ReValving System Caused by Enterococcus faecium Complicated by Iatrogenic Pancytopenia and Subacute Disseminated Intravascular Coagulation. J. Heart Valve Dis. 2015;24:130–132. - PubMed
-
- Habib G., Lancellotti P., Antunes M.J., Bongiorni M.G., Casalta J.P., Del Zotti F., Dulgheru R., El Khoury G., Erba P.A., Iung B., et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM) Eur. Heart J. 2015;36:3075–3128. doi: 10.1093/eurheartj/ehv319. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
