

Assessment of Intra-Abdominal Pressure with a Novel Continuous Bladder Pressure Monitor-A Clinical Validation Study
- PMID: 36836741
- PMCID: PMC9967253
- DOI: 10.3390/life13020384
Assessment of Intra-Abdominal Pressure with a Novel Continuous Bladder Pressure Monitor-A Clinical Validation Study
Abstract
Introduction: Intra-abdominal hypertension and the resulting abdominal compartment syndrome are serious complications of severely ill patients. Diagnosis requires an intra-abdominal pressure (IAP) measurement, which is currently cumbersome and underused. We aimed to test the accuracy of a novel continuous IAP monitor.
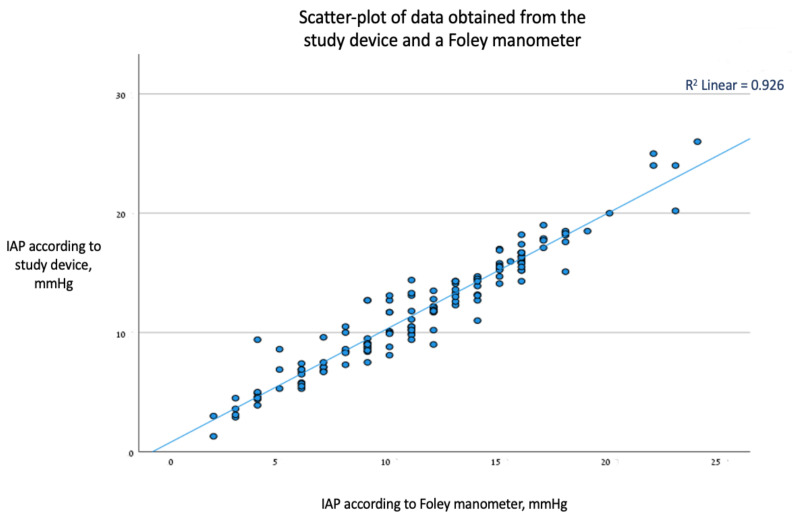
Methods: Adults having laparoscopic surgery and requiring urinary catheter intra-operatively were recruited to this single-arm validation study. IAP measurements using the novel monitor and a gold-standard foley manometer were compared. After anesthesia induction, a pneumoperitoneum was induced through a laparoscopic insufflator, and five randomly pre-defined pressures (between 5 and 25 mmHg) were achieved and simultaneously measured via both methods in each participant. Measurements were compared using Bland-Altman analysis.
Results: In total, 29 participants completed the study and provided 144 distinct pairs of pressure measurements that were analyzed. A positive correlation between the two methods was found (R2 = 0.93). There was good agreement between the methods, with a mean bias (95% CI) of -0.4 (-0.6, -0.1) mmHg and a standard deviation of 1.3 mmHg, which was statistically significant but of no clinical importance. The limits of agreement (where 95% of the differences are expected to fall) were -2.9 and 2.2 mmHg. The proportional error was statistically insignificant (p = 0.85), suggesting a constant agreement between the methods across the range of values tested. The percentage error was 10.7%.
Conclusions: Continuous IAP measurements using the novel monitor performed well in the clinical setup of controlled intra-abdominal hypertension across the evaluated range of pressures. Further studies should expand the range to more pathological values.
Keywords: abdominal compartment syndrome; foley manometer; intra-abdominal hypertension; intra-abdominal pressure monitoring.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures



References
LinkOut - more resources
Full Text Sources
Research Materials
