

Serum Uric Acid Predicts All-Cause and Cardiovascular Mortality Independently of Hypertriglyceridemia in Cardiometabolic Patients without Established CV Disease: A Sub-Analysis of the URic acid Right for heArt Health (URRAH) Study
- PMID: 36837863
- PMCID: PMC9959524
- DOI: 10.3390/metabo13020244
Serum Uric Acid Predicts All-Cause and Cardiovascular Mortality Independently of Hypertriglyceridemia in Cardiometabolic Patients without Established CV Disease: A Sub-Analysis of the URic acid Right for heArt Health (URRAH) Study
Abstract
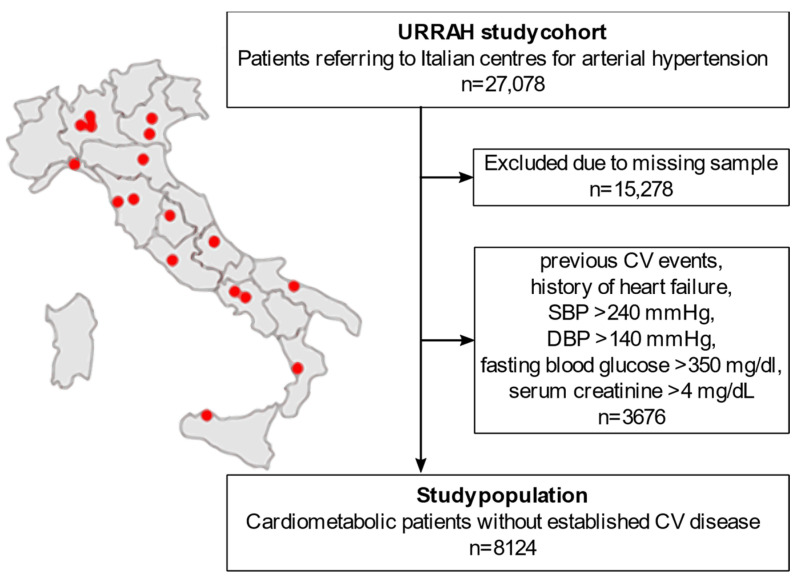
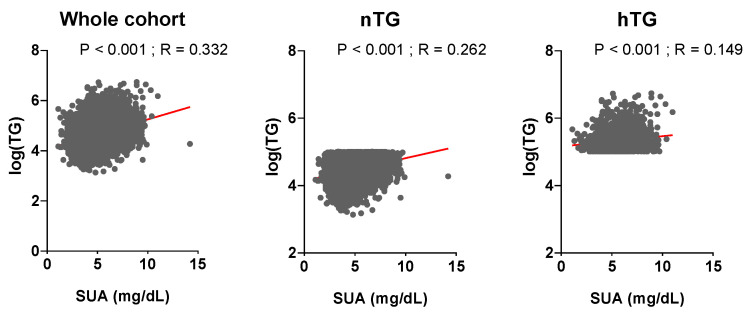
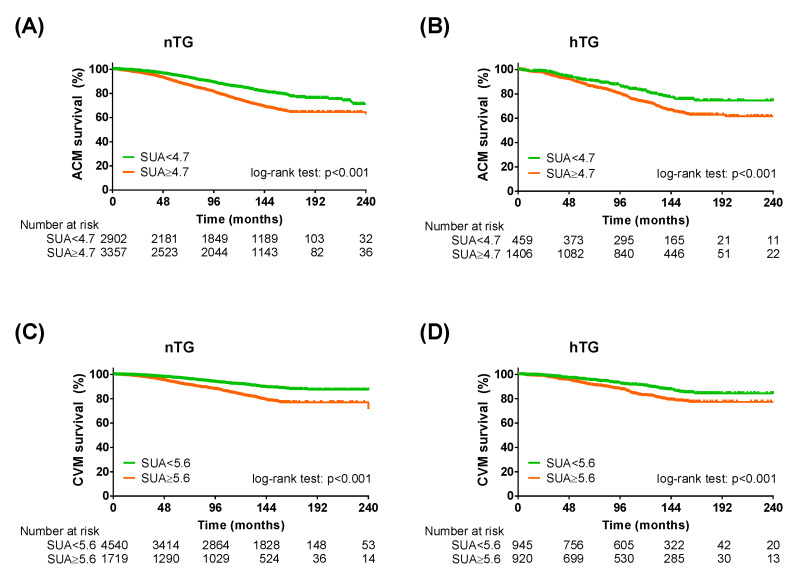
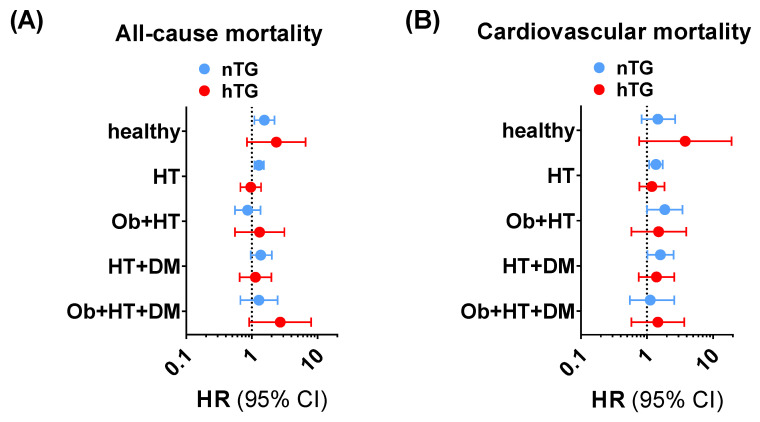
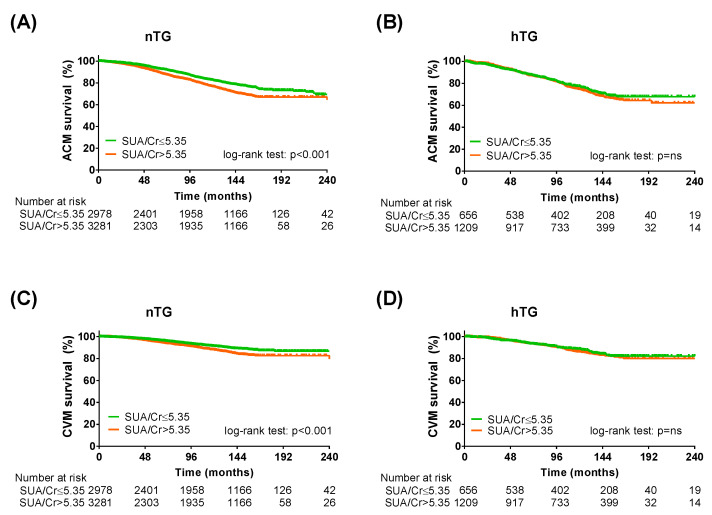
High serum uric acid (SUA) and triglyceride (TG) levels might promote high-cardiovascular risk phenotypes across the cardiometabolic spectrum. However, SUA predictive power in the presence of normal and high TG levels has never been investigated. We included 8124 patients from the URic acid Right for heArt Health (URRAH) study cohort who were followed for over 20 years and had no established cardiovascular disease or uncontrolled metabolic disease. All-cause mortality (ACM) and cardiovascular mortality (CVM) were explored by the Kaplan-Meier estimator and Cox multivariable regression, adopting recently defined SUA cut-offs for ACM (≥4.7 mg/dL) and CVM (≥5.6 mg/dL). Exploratory analysis across cardiometabolic subgroups and a sensitivity analysis using SUA/serum creatinine were performed as validation. SUA predicted ACM (HR 1.25 [1.12-1.40], p < 0.001) and CVM (1.31 [1.11-1.74], p < 0.001) in the whole study population, and according to TG strata: ACM in normotriglyceridemia (HR 1.26 [1.12-1.43], p < 0.001) and hypertriglyceridemia (1.31 [1.02-1.68], p = 0.033), and CVM in normotriglyceridemia (HR 1.46 [1.23-1.73], p < 0.001) and hypertriglyceridemia (HR 1.31 [0.99-1.64], p = 0.060). Exploratory and sensitivity analyses confirmed our findings, suggesting a substantial role of SUA in normotriglyceridemia and hypertriglyceridemia. In conclusion, we report that SUA can predict ACM and CVM in cardiometabolic patients without established cardiovascular disease, independent of TG levels.
Keywords: cardiometabolic; cardiovascular; hypertriglyceridemia; mortality; risk prediction; serum uric acid; triglycerides.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
