Relationship between Cytomegalovirus Viremia and Long-Term Outcomes in Kidney Transplant Recipients with Different Donor Ages
- PMID: 36838423
- PMCID: PMC9961719
- DOI: 10.3390/microorganisms11020458
Relationship between Cytomegalovirus Viremia and Long-Term Outcomes in Kidney Transplant Recipients with Different Donor Ages
Abstract
Objectives: To explore the Cytomegalovirus (CMV) burden on the long-term post-transplant course in different donor ages, we evaluated the incidence and risk factors for CMV in our kidney-transplanted patients (KTs) with extensive adoption of expanded-criteria donors (ECDs).
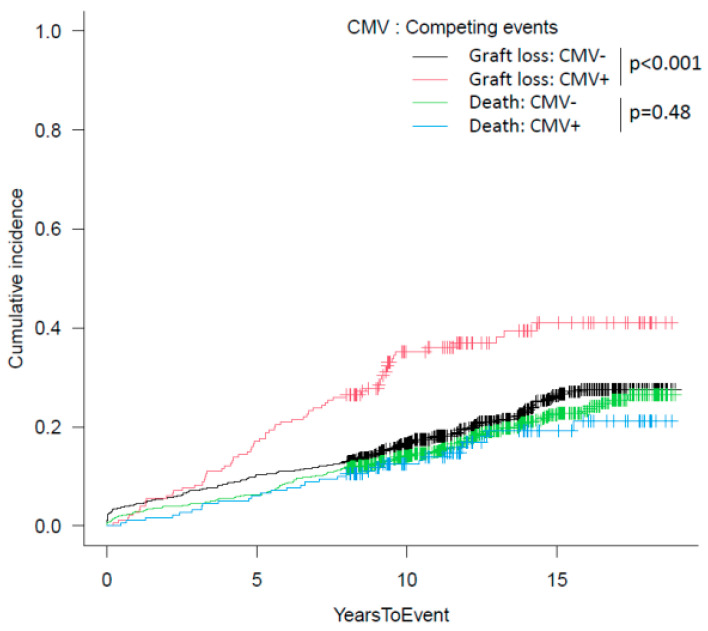
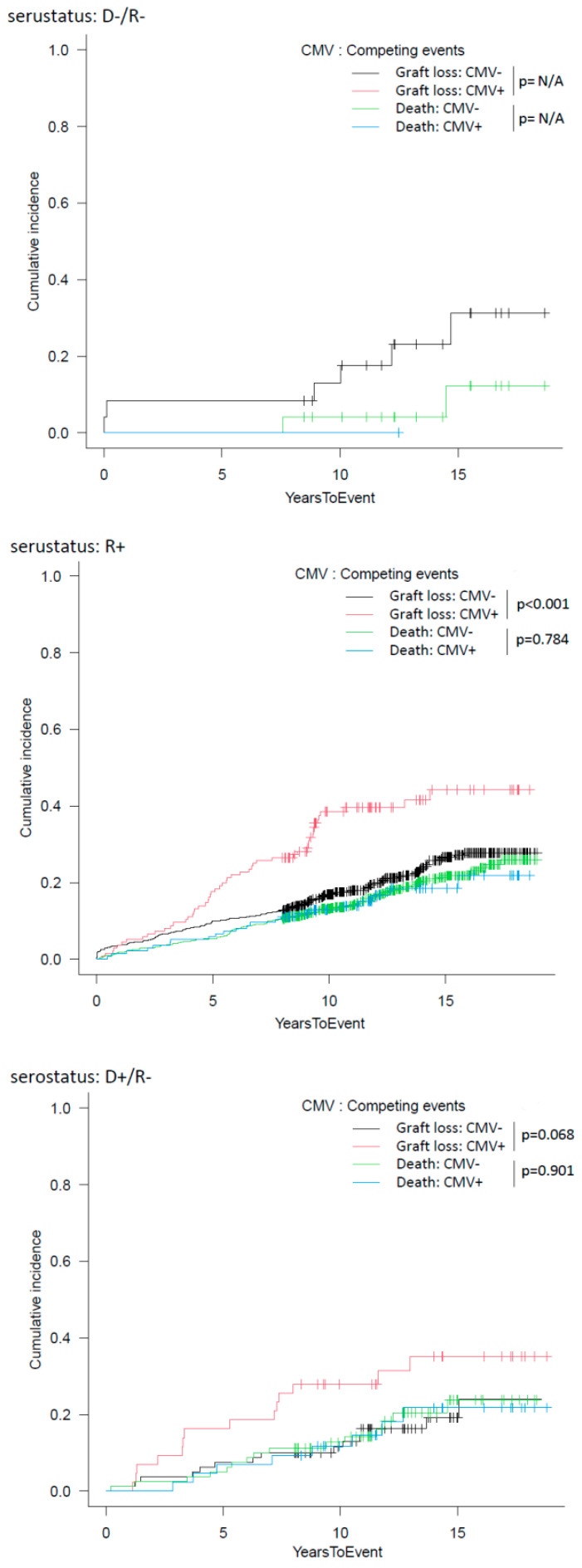
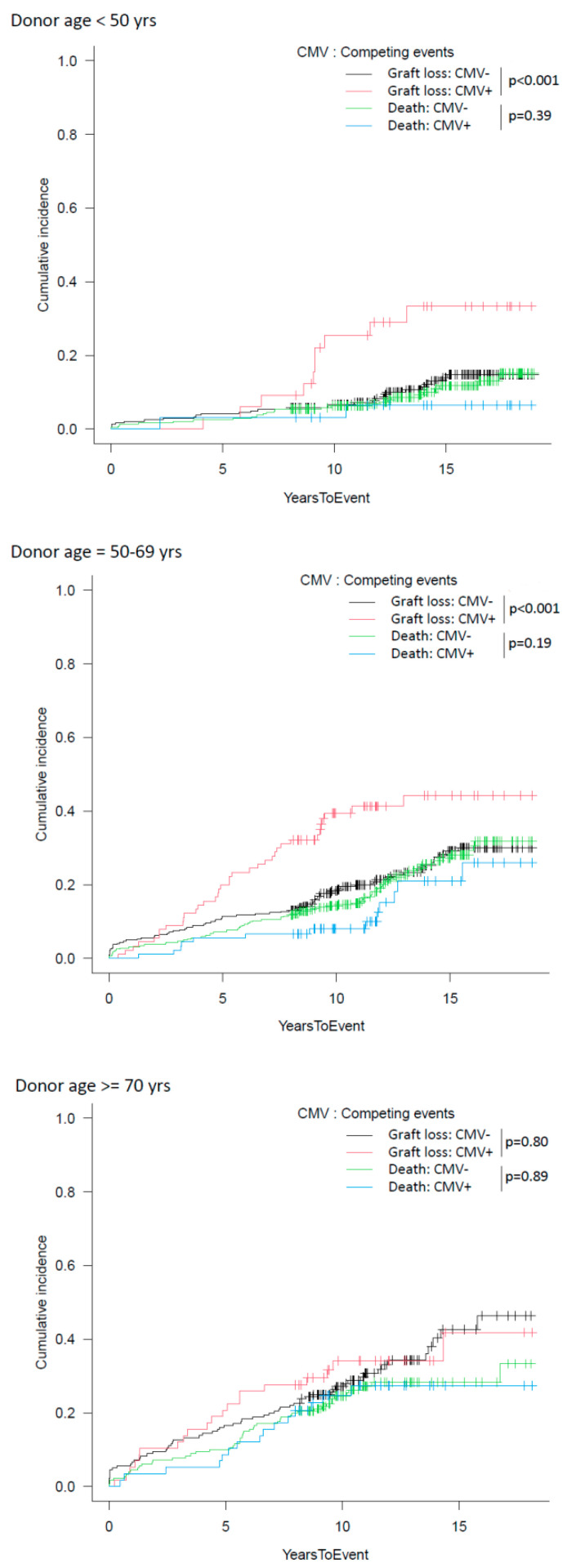
Methods: Retrospective evaluation of 929 consecutive first KTs (49.5% receiving an organ from a donor ≥ 60 years) performed between 01-2003 and 12-2013. Overall survival was estimated using Kaplan-Meier curves; cumulative incidence function was additionally analyzed to consider the potential role of death with a functioning graft as a competitive event with graft dysfunction and to avoid overestimation. Apart from regular DNAemia monitoring in all patients, prophylaxis was adopted in high-risk groups (D+/R- or recipients of anti-thymocyte globulin induction), with pre-emptive therapy in the remaining groups.
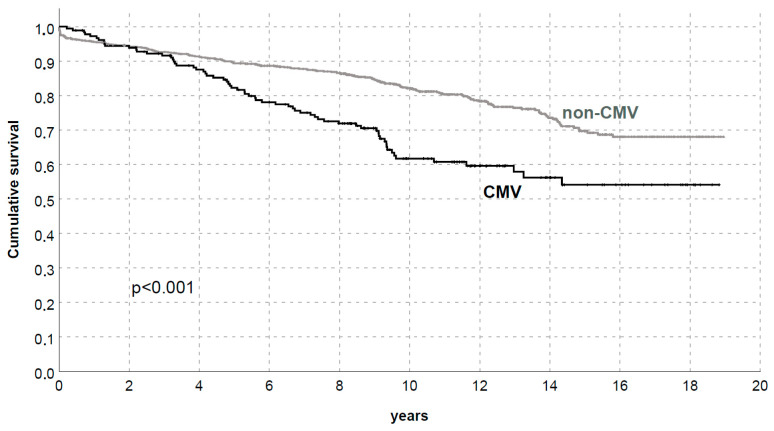
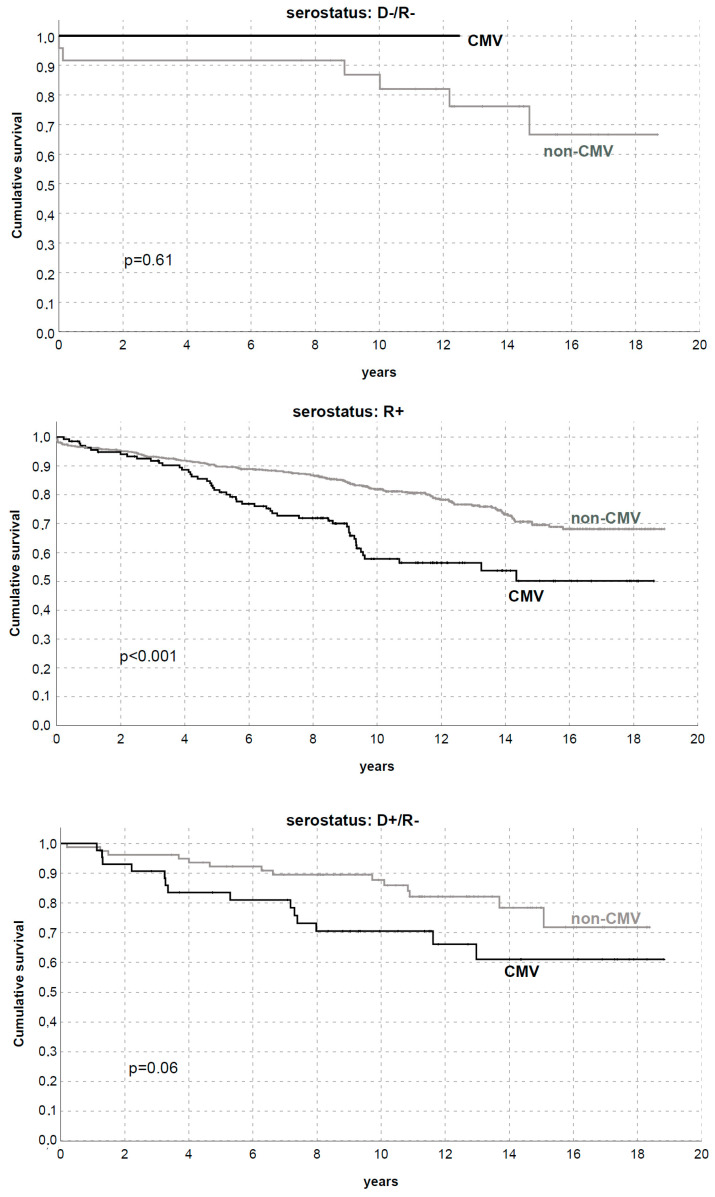
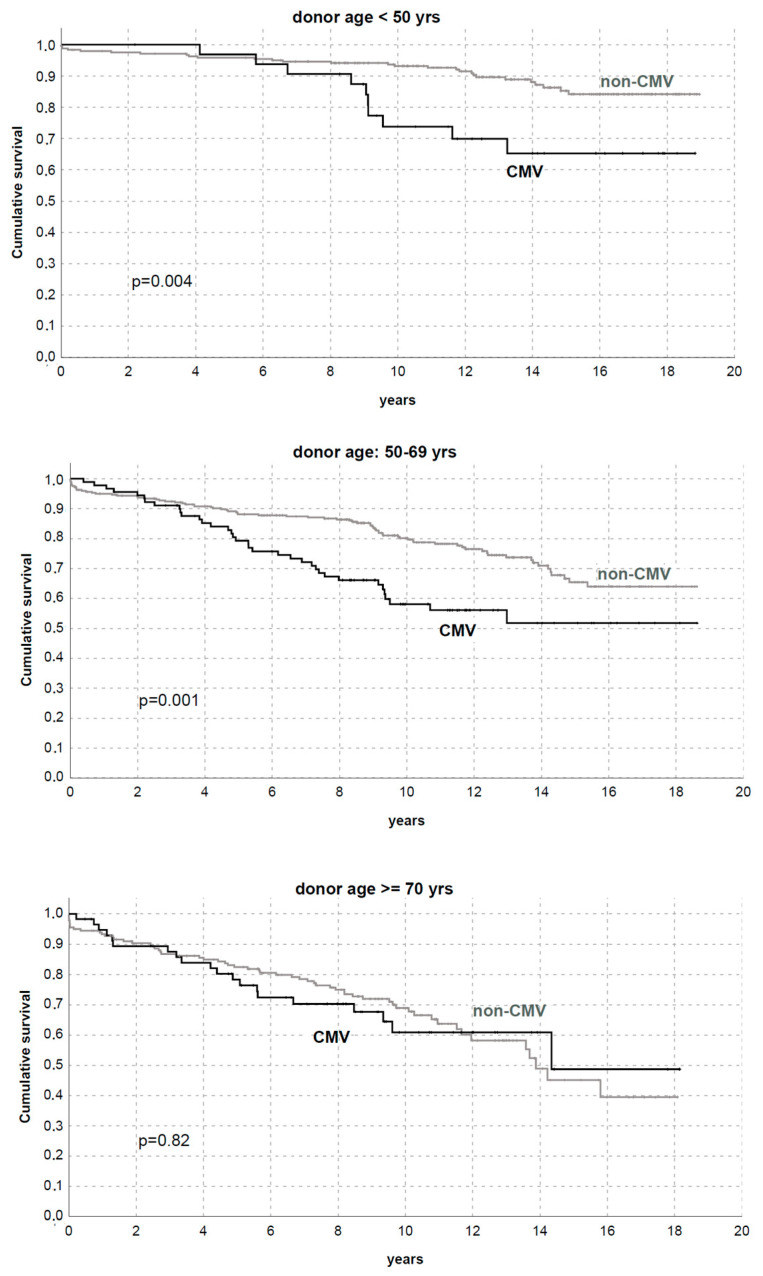
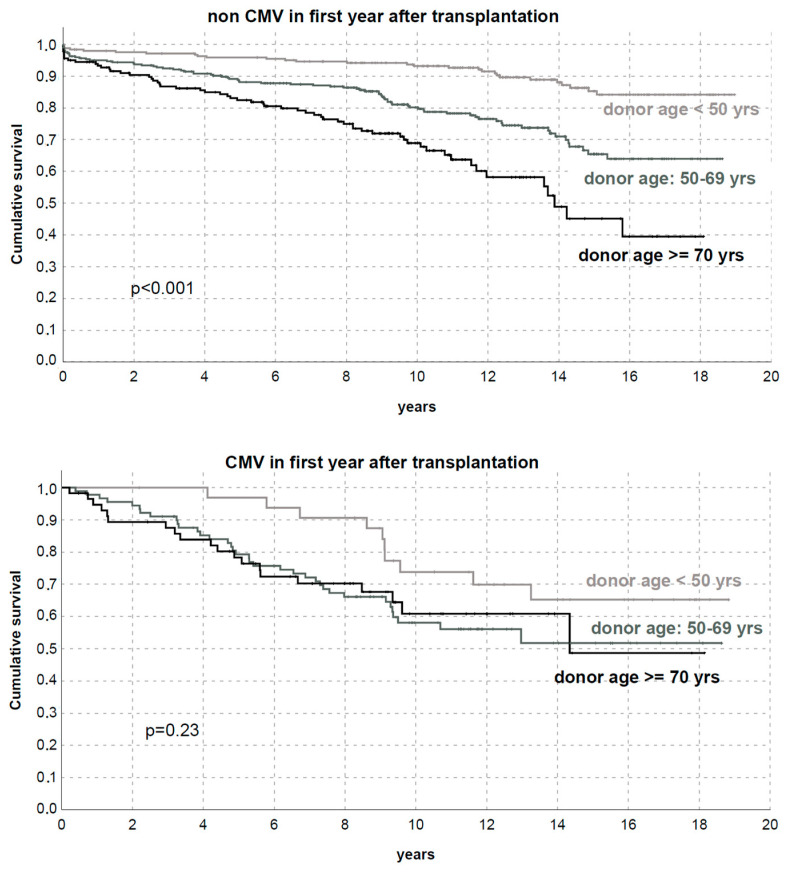
Results: CMV incidence was 19.5% (4-34.9% according to serostatus combination: D-/R-, D-/R+, D+/R+, D+/R-). Donor and recipient age, recipient pre-transplant hypertension, DR antigen compatibility, cold ischemia time, and post-transplant early complications, including rejection, urologic and renal artery stenosis, and lower renal function and proteinuria ≥ 0.5 g/day at one year after KT were associated with CMV. CMV determined lower death-censored graft survival (DCGS) (p < 0.01), with a prominent effect in R+ (p < 0.01) and without impact in R- (p = 0.32 in D-/R- and p = 0.006 in D+/R-). Interestingly, CMV occurrence influenced DCGS only in KTs who received grafts from donors < 50 or 50-69 years old (p < 0.01), while it was not significant with older donors (p = 0.07). The analysis of the cumulative incidence of graft loss accounting for death as a competing risk confirmed all these findings. In multivariate analysis, CMV replication/disease in the first year was an independent predictor for DCGS (HR 1.73 [1.3-2.3]).
Conclusions: In a large population with extensive ECD adoption, CMV viremia in the first year demonstrates its harmful effect with an independent role for graft loss and significant impact among R+ recipients and KTs with donors < 70 years.
Keywords: cumulative incidence function; cytomegalovirus; donor age; long-term outcomes; renal transplantation; risk factors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures