

Pediatric Mini-Tablets: Predicting the Hidden Risk of Fill Errors
- PMID: 36839916
- PMCID: PMC9961976
- DOI: 10.3390/pharmaceutics15020594
Pediatric Mini-Tablets: Predicting the Hidden Risk of Fill Errors
Abstract
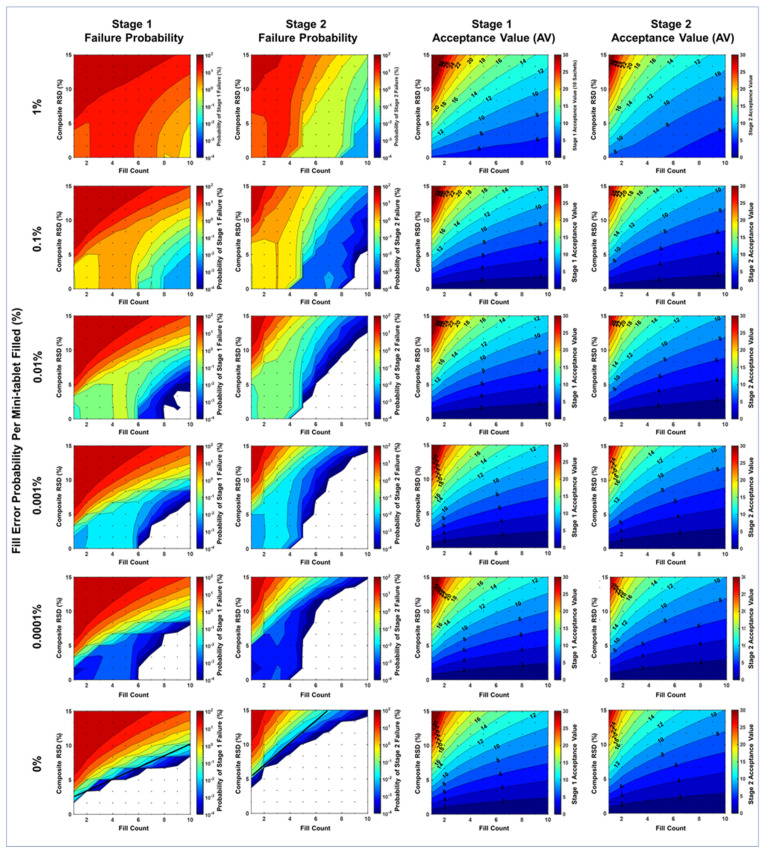
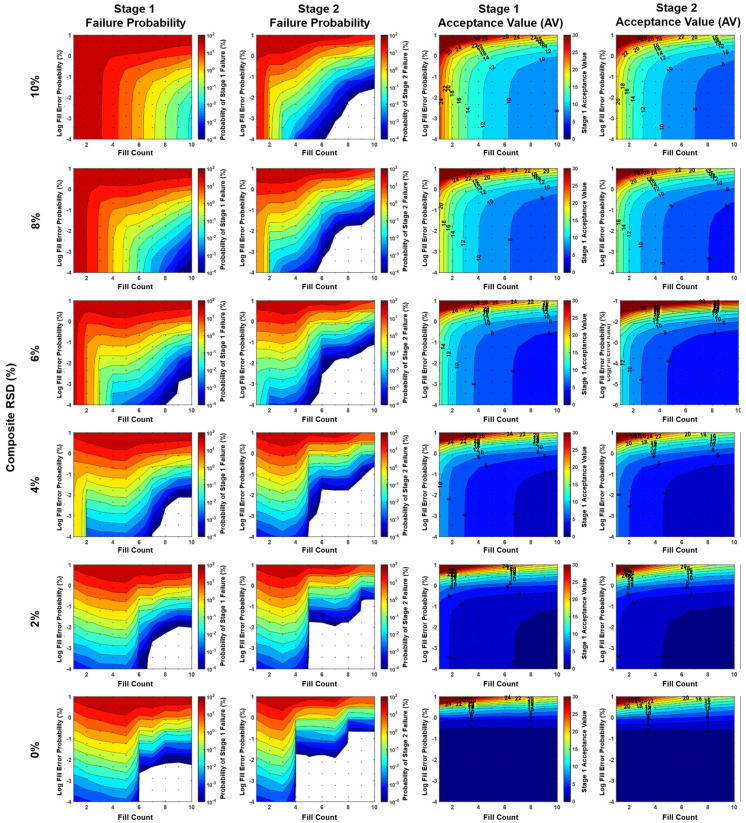
Compressed mini-tablets in sachets or capsules are an increasingly prevalent oral solid dosage form for pediatric products. While resembling adult tablets, additional care is required to control weight and potency (blend uniformity) variation due to their small size (≤2.5 mm average diameter). Additionally, sachet fill count errors complicate dose accuracy as they are difficult to resolve with weight-checking equipment. This study quantified the probability of failing content uniformity (CU) specifications (which results in the inability to release a batch) defined in USP <905> using a Monte Carlo computational model. Failure risk was modeled as a function of sachet fill count, mini-tablet weight, potency distribution, and fill error frequency. The model allows product developers to (1) determine appropriate fill counts based on anticipated product weight and potency relative standard deviation (RSD), (2) set fill error probability tolerances for sachet filling processes, (3) identify CU improvement opportunities, and (4) quantify the probability of CU failure informing risk management activities and risk disclosure for regulatory agencies. A representative product with weight and potency RSD no greater than 5%, fill count of 1-4 mini-tablets per sachet, and fill error probability per mini-tablet filled of 0.1% may experience CU batch failure probabilities as high as 8.23%, but only 0.283% if the fill count is increased to 5-10 mini-tablets per sachet. Generally, fill counts of less than five mini-tablets per sachet should be avoided where possible.
Keywords: content uniformity; dose uniformity; fill count; fill errors; mini-tablet; sachet.
Conflict of interest statement
The authors are employees of a company involved in research and commercialization of pediatric pharmaceutical products. Brandon G. Gerberich is an inventor on patent applications pertaining to this research.
Figures





Similar articles
-
Evaluation of the Discrepancy between the European Pharmacopoeia Test and an Adopted United States Pharmacopoeia Test Regarding the Weight Uniformity of Scored Tablet Halves: Is Harmonization Required?PDA J Pharm Sci Technol. 2012 Jan-Feb;66(1):20-7. doi: 10.5731/pdajpst.2012.00791. PDA J Pharm Sci Technol. 2012. PMID: 22307659
-
Understanding die fill variation during mini-tablet production.Int J Pharm. 2017 Dec 20;534(1-2):279-286. doi: 10.1016/j.ijpharm.2017.10.042. Epub 2017 Oct 24. Int J Pharm. 2017. PMID: 29074390
-
Dose Uniformity of Scored and Unscored Tablets: Application of the FDA Tablet Scoring Guidance for Industry.PDA J Pharm Sci Technol. 2016 11/12;70(6):523-532. doi: 10.5731/pdajpst.2016.006411. PDA J Pharm Sci Technol. 2016. PMID: 27974592
-
Blend Segregation in Tablets Manufacturing and Its Effect on Drug Content Uniformity-A Review.Pharmaceutics. 2021 Nov 11;13(11):1909. doi: 10.3390/pharmaceutics13111909. Pharmaceutics. 2021. PMID: 34834324 Free PMC article. Review.
-
Pediatric Oral Formulations: An Updated Review of Commercially Available Pediatric Oral Formulations Since 2007.J Pharm Sci. 2019 Apr;108(4):1335-1365. doi: 10.1016/j.xphs.2018.11.013. Epub 2018 Nov 14. J Pharm Sci. 2019. PMID: 30447227 Review.
References
-
- Regulation (EC) No 1901/2006 of the European Parliament and of the Council of 12 December 2006 on medicinal products for paediatric use and amending Regulation (EEC) No 1768/92, Directive 2001/20/EC, Directive 2001/83/EC and Regulation (EC) No 726/2004. Off. J. Eur. Union. 2006;378:1–19.
-
- Tumuluri V. Drug Delivery Trends. Elsevier; Amsterdam, The Netherlands: 2020. Pharmaceutical mini-tablets: A revived trend; pp. 123–139.
LinkOut - more resources
Full Text Sources
