

Excess mortality among non-COVID-19 surgical patients attributable to the exposure of French intensive and intermediate care units to the pandemic
- PMID: 36840798
- PMCID: PMC9959950
- DOI: 10.1007/s00134-023-07000-3
Excess mortality among non-COVID-19 surgical patients attributable to the exposure of French intensive and intermediate care units to the pandemic
Abstract
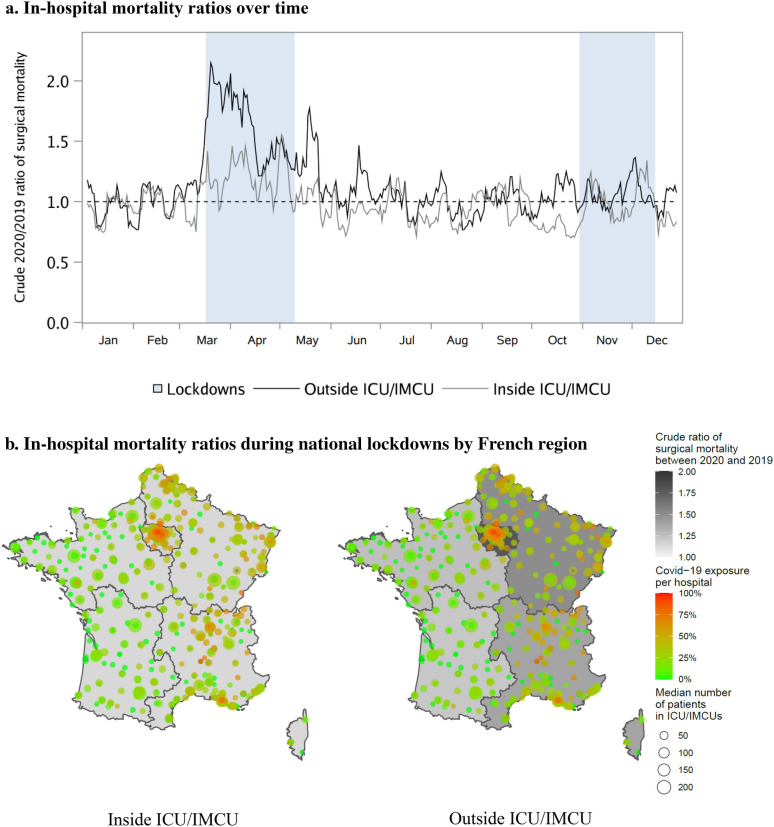
Purpose: The mobilization of most available hospital resources to manage coronavirus disease 2019 (COVID-19) may have affected the safety of care for non-COVID-19 surgical patients due to restricted access to intensive or intermediate care units (ICU/IMCUs). We estimated excess surgical mortality potentially attributable to ICU/IMCUs overwhelmed by COVID-19, and any hospital learning effects between two successive pandemic waves.
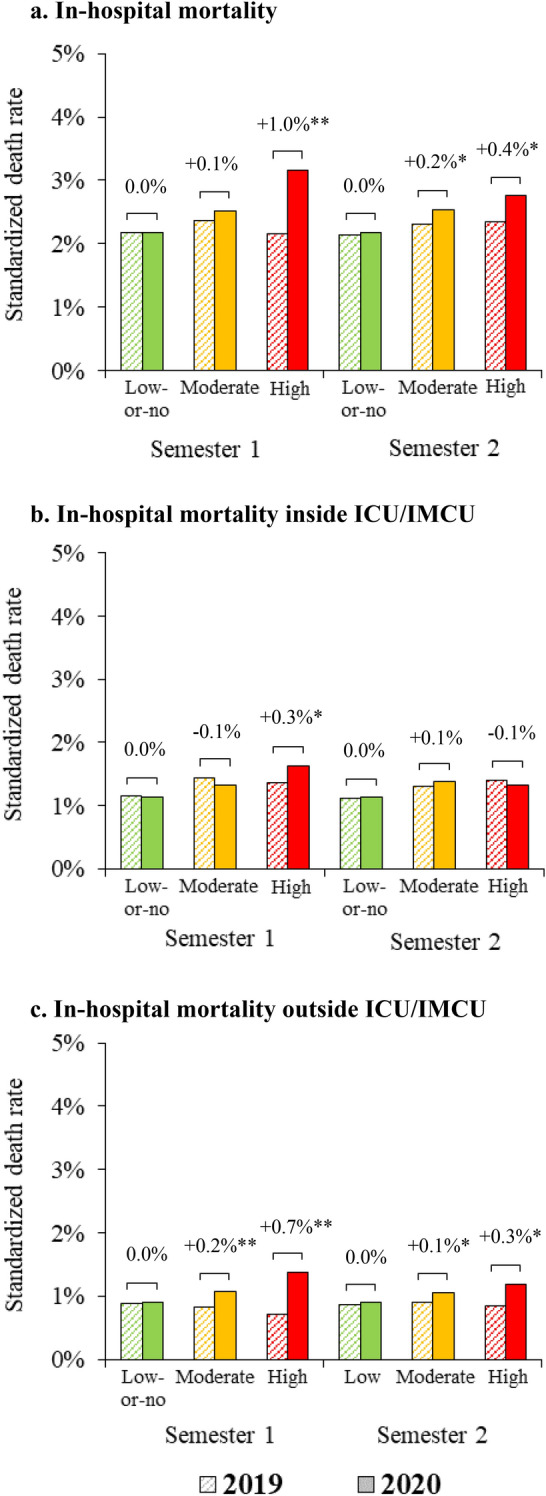
Methods: This nationwide observational study included all patients without COVID-19 who underwent surgery in France from 01/01/2019 to 31/12/2020. We determined pandemic exposure of each operated patient based on the daily proportion of COVID-19 patients among all patients treated within the ICU/IMCU beds of the same hospital during his/her stay. Multilevel models, with an embedded triple-difference analysis, estimated standardized in-hospital mortality and compared mortality between years, pandemic exposure groups, and semesters, distinguishing deaths inside or outside the ICU/IMCUs.
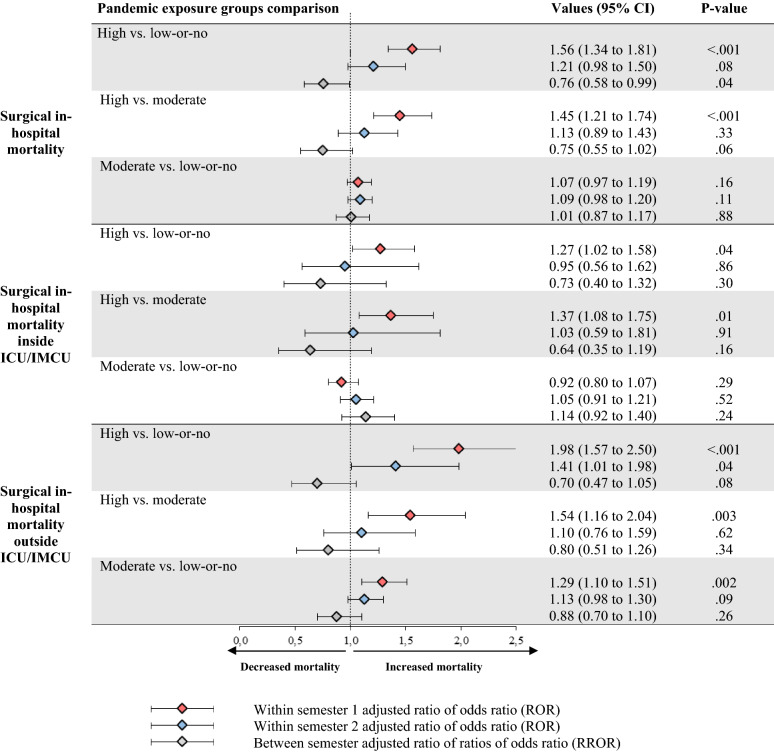
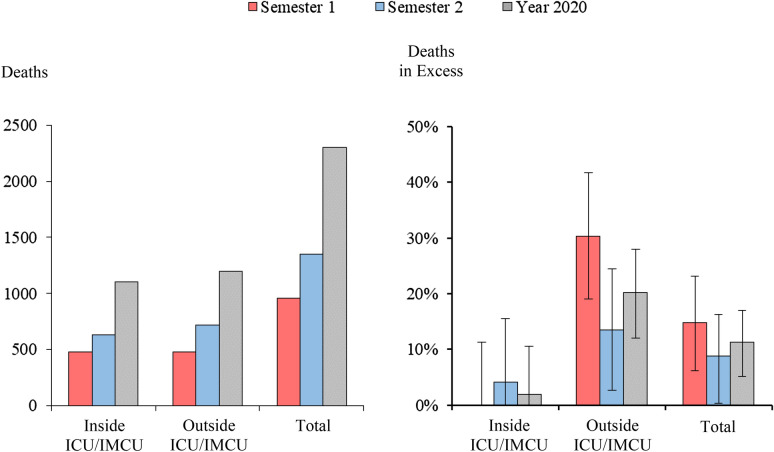
Results: Of 1,870,515 non-COVID-19 patients admitted for surgery in 655 hospitals, 2% died. Compared to 2019, standardized mortality increased by 1% (95% CI 0.6-1.4%) and 0.4% (0-1%) during the first and second semesters of 2020, among patients operated in hospitals highly exposed to pandemic. Compared to the low-or-no exposure group, this corresponded to a higher risk of death during the first semester (adjusted ratio of odds-ratios 1.56, 95% CI 1.34-1.81) both inside (1.27, 1.02-1.58) and outside the ICU/IMCU (1.98, 1.57-2.5), with a significant learning effect during the second semester compared to the first (0.76, 0.58-0.99).
Conclusion: Significant excess mortality essentially occurred outside of the ICU/IMCU, suggesting that access of surgical patients to critical care was limited.
Keywords: COVID-19; Critical care; Patient safety; Surgical mortality.
© 2023. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
All the authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
