

Intergenerational transmission of the effects of maternal exposure to childhood maltreatment in the USA: a retrospective cohort study
- PMID: 36841563
- PMCID: PMC9982823
- DOI: 10.1016/S2468-2667(23)00025-7
Intergenerational transmission of the effects of maternal exposure to childhood maltreatment in the USA: a retrospective cohort study
Abstract
Background: Childhood maltreatment is associated with adverse health outcomes and this risk can be transmitted to the next generation. We aimed to investigate the association between exposure to maternal childhood maltreatment and common childhood physical and mental health problems, neurodevelopmental disorders, and related comorbidity patterns in offspring.
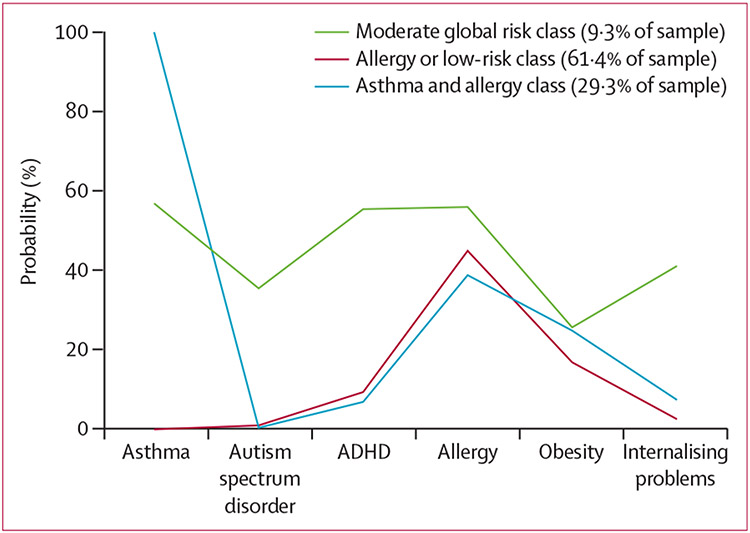
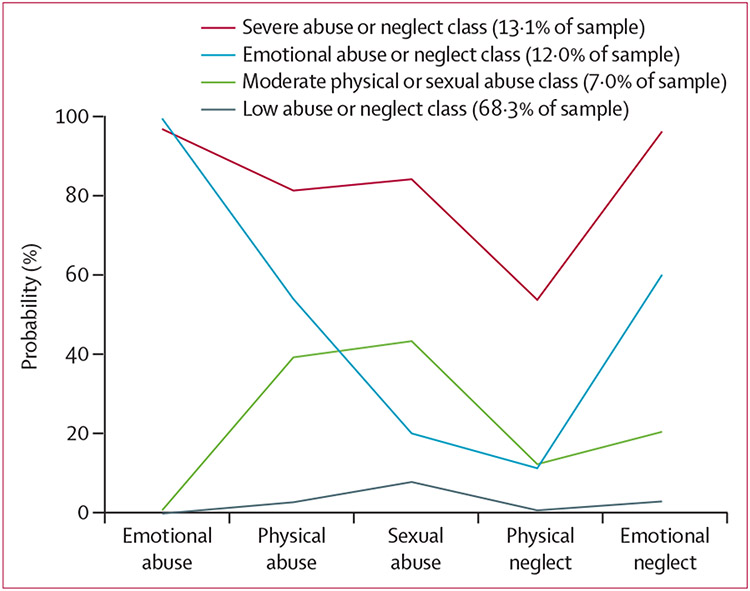
Methods: We conducted a retrospective cohort study using data from the Environmental influences on Child Health Outcomes (ECHO) Program, which was launched to investigate the influence of early life exposures on child health and development in 69 cohorts across the USA. Eligible mother-child dyads were those with available data on maternal childhood maltreatment exposure and at least one child health outcome measure (autism spectrum disorder, attention-deficit hyperactivity disorder [ADHD], internalising problems, obesity, allergy, and asthma diagnoses). Maternal history of childhood maltreatment was obtained retrospectively from the Adverse Childhood Experiences or Life Stressor Checklist questionnaires. We derived the prevalence of the specified child health outcome measures in offspring across childhood and adolescence by harmonising caregiver reports and other relevant sources (such as medical records) across cohorts. Child internalising symptoms were assessed using the Child Behavior Checklist. Associations between maternal childhood maltreatment and childhood health outcomes were measured using a series of mixed-effects logistic regression models. Covariates included child sex (male or female), race, and ethnicity; maternal and paternal age; maternal education; combined annual household income; maternal diagnosis of depression, asthma, ADHD, allergy, or autism spectrum disorder; and maternal obesity. Two latent class analyses were conducted: to characterise patterns of comorbidity of child health outcomes; and to characterise patterns of co-occurrence of childhood maltreatment subtypes. We then investigated the association between latent class membership and maternal childhood maltreatment and child health outcomes, respectively.
Findings: Our sample included 4337 mother-child dyads from 21 longitudinal cohorts (with data collection initiated between 1999 and 2016). Of 3954 mothers in the study, 1742 (44%) had experienced exposure to abuse or neglect during their childhood. After adjustment for confounding, mothers who experienced childhood maltreatment were more likely to have children with internalising problems in the clinical range (odds ratio [OR] 2·70 [95% CI 1·95-3·72], p<0·0001), autism spectrum disorder (1·70 [1·13-2·55], p=0·01), ADHD (2·09 [1·63-2·67], p<0·0001), and asthma (1·54 [1·34-1·77], p<0·0001). In female offspring, maternal childhood maltreatment was associated with a higher prevalence of obesity (1·69 [1·17-2·44], p=0·005). Children of mothers exposed to childhood maltreatment were more likely to exhibit a diagnostic pattern characterised by higher risk for multimorbidity. Exposure to multiple forms of maltreatment across all subtypes of maternal childhood maltreatment was associated with the highest risk increases for most offspring health outcomes, suggesting a dose-response relationship.
Interpretation: Our findings suggest that maternal childhood maltreatment experiences can be a risk factor for disease susceptibility in offspring across a variety of outcomes and emphasise the need for policies focusing on breaking the intergenerational transmission of adversity.
Funding: Environmental influences on Child Health Outcomes Program, Office of the Director, National Institutes of Health.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests CSD, AEH, HNS, TGO, RKM, CB, ESB, EO, CKB, MBE, RJW, SCLD, TMB, NRB, and JP report funding from the National Institutes of Health (NIH). RKM reports research support from the Health Resources and Services Administration and the New York State Department of Health and participation as Chair of the Scientific Advisory Committee for the GlaxoSmithKline Bieimumab Pregnancy Registry. SCLD reports consulting fees from Nestlé Nutrition. JP reports research support from Takeda (formerly Shire) and Aevi Genomics and consulting fees from Innovative Science. ESB reports honoria from the NIH Study Sections. All other authors declare no competing interests.
Figures
Comment in
-
Intergenerational links between childhood maltreatment and health outcomes in offspring.Lancet Public Health. 2023 Mar;8(3):e170-e171. doi: 10.1016/S2468-2667(23)00035-X. Lancet Public Health. 2023. PMID: 36841557 No abstract available.
References
-
- Walker EA, Unutzer J, Rutter C, et al. Costs of health care use by women HMO members with a history of childhood abuse and neglect. Arch Gen Psychiatry 1999; 56: 609–13. - PubMed
-
- Stoltenborgh M, Bakermans-Kranenburg MJ, Alink LRA, van IJzendoorn MH. The prevalence of child maltreatment across the globe: review of a series of meta-analyses. Child Abuse Rev 2015; 24: 37–50.
-
- Leeb R, Paulozzi L, Melanson C, Simon T, Arias I. Child maltreatment surveillance: uniform definitions for public health and recommended data elements. Atlanta, GA: Centers for Disease Control and Prevention, 2008. https://www.cdc.gov/violenceprevention/pdf/cm_surveillance-a.pdf (accessed Nov 17, 2020).
-
- The Lancet Public Health. Childhood adversity: a profound determinant of health. Lancet Public Health 2021; 6: e780. - PubMed
Publication types
MeSH terms
Grants and funding
- UH3 OD023332/OD/NIH HHS/United States
- K23 AI159144/AI/NIAID NIH HHS/United States
- UH3 OD023389/OD/NIH HHS/United States
- U2C OD023375/OD/NIH HHS/United States
- UG3 OD023320/OD/NIH HHS/United States
- UH3 OD023287/OD/NIH HHS/United States
- U24 OD023319/OD/NIH HHS/United States
- UH3 OD023305/OD/NIH HHS/United States
- UG3 OD023313/OD/NIH HHS/United States
- UG3 OD023282/OD/NIH HHS/United States
- UH3 OD023288/OD/NIH HHS/United States
- UH3 OD023342/OD/NIH HHS/United States
- R01 HD034568/HD/NICHD NIH HHS/United States
- UH3 OD023337/OD/NIH HHS/United States
- UH3 OD023328/OD/NIH HHS/United States
- U24 OD023382/OD/NIH HHS/United States
- UH3 OD023313/OD/NIH HHS/United States
- UH3 OD023289/OD/NIH HHS/United States
- U24 ES028533/ES/NIEHS NIH HHS/United States
- UH3 OD023286/OD/NIH HHS/United States
- UG3 OD023244/OD/NIH HHS/United States
- UH3 OD023271/OD/NIH HHS/United States
- UH3 OD023282/OD/NIH HHS/United States
- UG3 OD023271/OD/NIH HHS/United States
- UH3 OD023244/OD/NIH HHS/United States
- UH3 OD023320/OD/NIH HHS/United States
- R24 ES028533/ES/NIEHS NIH HHS/United States
- UH3 OD023349/OD/NIH HHS/United States
