

Combination of exercise and GLP-1 receptor agonist treatment reduces severity of metabolic syndrome, abdominal obesity, and inflammation: a randomized controlled trial
- PMID: 36841762
- PMCID: PMC9960425
- DOI: 10.1186/s12933-023-01765-z
Combination of exercise and GLP-1 receptor agonist treatment reduces severity of metabolic syndrome, abdominal obesity, and inflammation: a randomized controlled trial
Abstract
Background: Identifying and reducing cardiometabolic risks driven by obesity remains a healthcare challenge. The metabolic syndrome is associated with abdominal obesity and inflammation and is predictive of long-term risk of developing type 2 diabetes and cardiovascular disease in otherwise healthy individuals living with obesity. Therefore, we investigated the effects of adherent exercise, a glucagon-like peptide 1 receptor agonist (GLP-1 RA), or the combination on severity of metabolic syndrome, abdominal obesity, and inflammation following weight loss.
Methods: This was a randomized, double-blinded, placebo-controlled trial. During an 8-week low-calorie diet (800 kcal/day), 195 adults with obesity and without diabetes lost 12% in body weight. Participants were then evenly randomized to four arms of one-year treatment with: placebo, moderate-to-vigorous exercise (minimum of 150 min/week of moderate-intensity or 75 min/week of vigorous-intensity aerobic physical activity or an equivalent combination of both), the GLP-1 RA liraglutide 3.0 mg/day, or a combination (exercise + liraglutide). A total of 166 participants completed the trial. We assessed the prespecified secondary outcome metabolic syndrome severity z-score (MetS-Z), abdominal obesity (estimated as android fat via dual-energy X-ray absorptiometry), and inflammation marker high-sensitivity C-reactive protein (hsCRP). Statistical analysis was performed on 130 participants adherent to the study interventions (per-protocol population) using a mixed linear model.
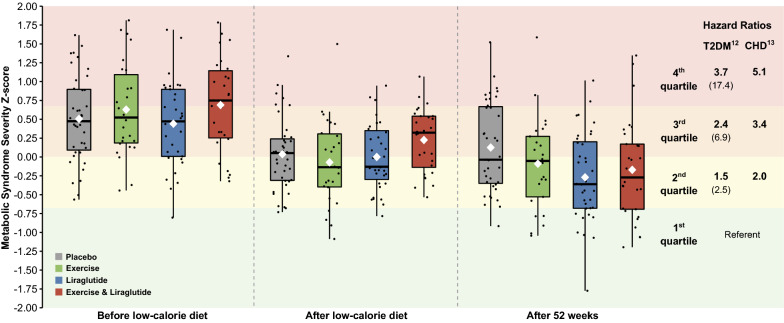
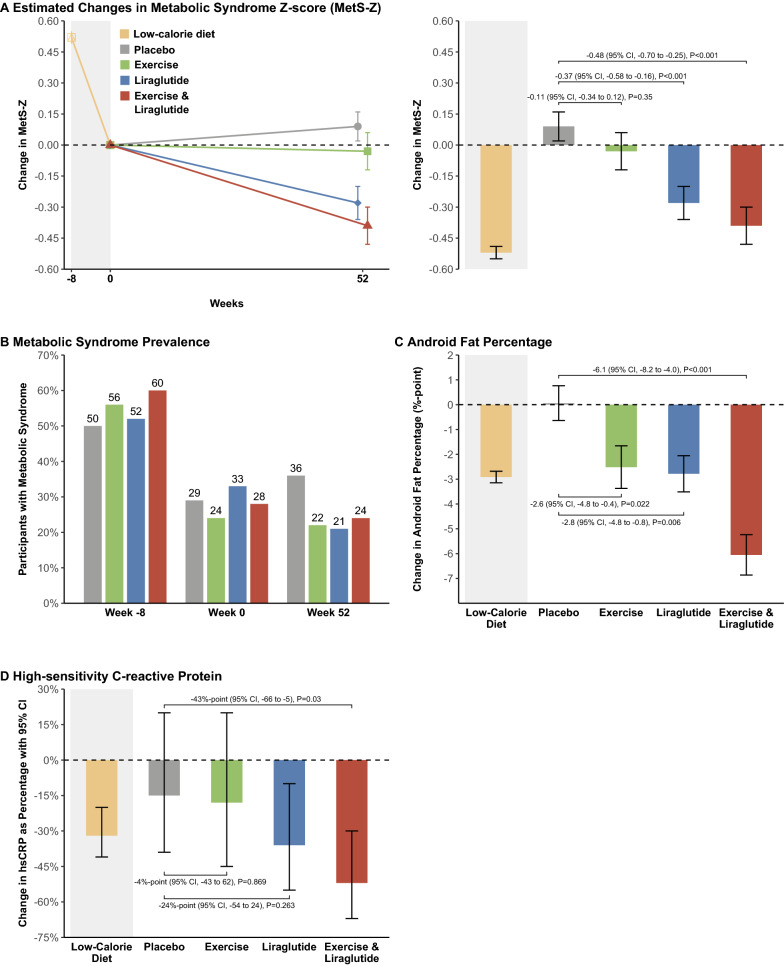
Results: The diet-induced weight loss decreased the severity of MetS-Z from 0.57 to 0.06, which was maintained in the placebo and exercise groups after one year. MetS-Z was further decreased by liraglutide (- 0.37, 95% CI - 0.58 to - 0.16, P < 0.001) and the combination treatment (- 0.48, 95% CI - 0.70 to - 0.25, P < 0.001) compared to placebo. Abdominal fat percentage decreased by 2.6, 2.8, and 6.1 percentage points in the exercise, liraglutide, and combination groups compared to placebo, respectively, and hsCRP decreased only in the combination group compared with placebo (by 43%, P = 0.03).
Conclusion: The combination of adherent exercise and liraglutide treatment reduced metabolic syndrome severity, abdominal obesity, and inflammation and may therefore reduce cardiometabolic risk more than the individual treatments. Trial registration EudraCT number: 2015-005585-32, ClinicalTrials.gov: NCT04122716.
Keywords: Cardiometabolic risk; Exercise; GLP-1; Inflammation; Metabolic syndrome; Obesity; Randomized clinical trial.
© 2023. The Author(s).
Conflict of interest statement
RMS: Family member holds Novo Nordisk stocks. MR: Currently employed at Novo Nordisk. JJH: Advisory boards: Novo Nordisk. SM: Advisory boards: AstraZeneca; Boehringer Ingelheim; Eli Lilly; Merck Sharp & Dohme; Novo Nordisk; Sanofi Aventis. Lecture fees: AstraZeneca; Boehringer Ingelheim; Merck Sharp & Dohme; Novo Nordisk; Sanofi Aventis. Grant Recipient: Novo Nordisk, Boehringer-Ingelheim. SST: Grant and lecture fee recipient, Novo Nordisk. JRL, CJ, CRJ, SBKJ, MBB, AFB, LG, JBJ, CA, BMS have no disclosures.
Figures
References
-
- Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the obesity society. J Am Coll Cardiol. 2014;63(25):2985–3023. doi: 10.1016/j.jacc.2013.11.004. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
