Comorbidities in autism spectrum disorder and their etiologies
- PMID: 36841830
- PMCID: PMC9958310
- DOI: 10.1038/s41398-023-02374-w
Comorbidities in autism spectrum disorder and their etiologies
Abstract
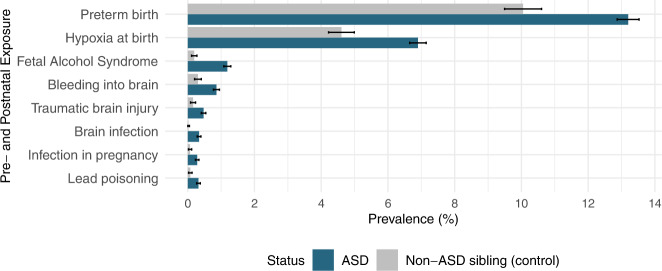
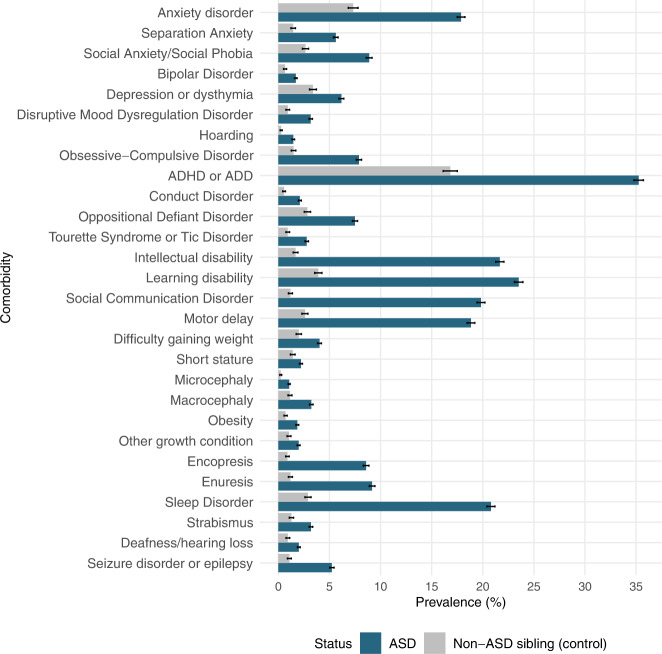
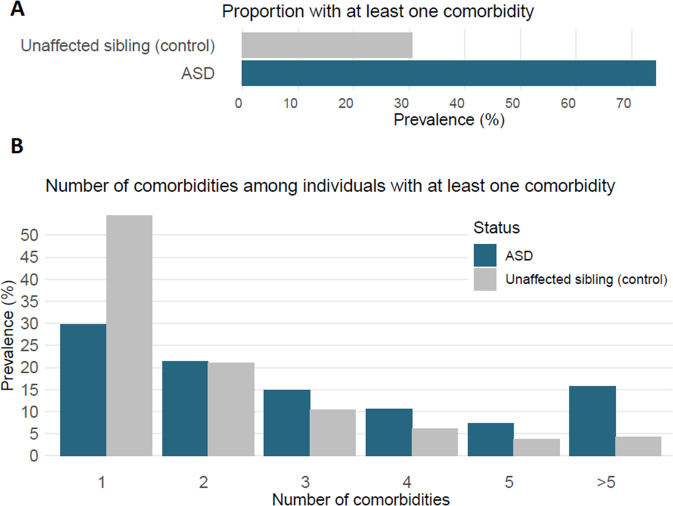
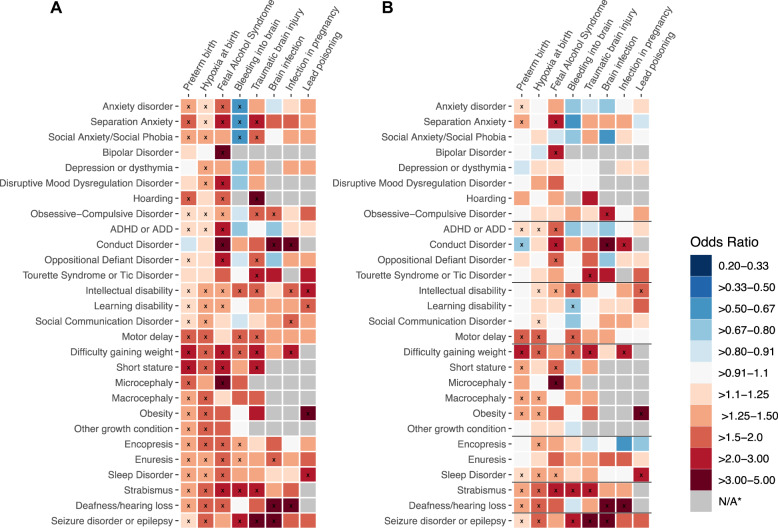
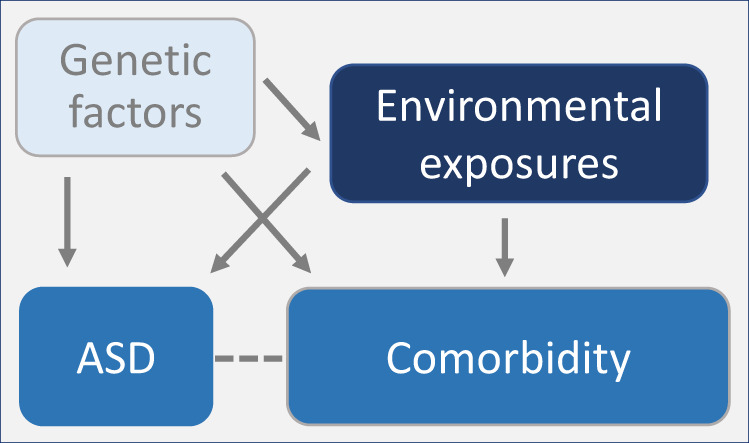
Individuals with autism spectrum disorder (ASD), in addition to the core features of the disease, experience a higher burden of co-occurring medical conditions. This study sought to describe the frequency and distribution of comorbidit conditions in individuals with ASD, and systematically evaluate the possibility that pre- and postnatal exposures (e.g., preterm birth, hypoxia at birth, traumatic brain injury, and fetal alcohol syndrome) associated with ASD may also be linked with distinct comorbidities. We used the SPARK study database, launched by the Simons Foundation Autism Research Initiative (SFARI). Comorbidities considered in the study included neurological, cognitive, psychiatric, and physical conditions. The study sample consisted of 42,569 individuals with ASD and their 11,389 non-ASD siblings (full and half siblings). Majority (74%) of individuals with ASD had at least one comorbidity, and had a greater average number of comorbidities than their non-ASD siblings. Preterm birth and hypoxia at birth were the most common peri-natal exposures in the sample. In logistic regression models adjusted for covariates, these exposures were associated with several distinct comorbidities in ASD cases, including attention and behavior problems, psychiatric and neurological disorders, and growth conditions. A similar pattern of association was also observed in non-ASD siblings. Our findings underscore that individuals with ASD experience a greater burden of comorbidities, which could be partly attributable to the higher rates of perinatal exposures compared to their non-ASD siblings. Study findings, if replicated in other samples, can inform the etiology of comorbidity in ASD.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures