

Cost-Utility Analysis of Deep Learning and Trained Human Graders for Diabetic Retinopathy Screening in a Nationwide Program
- PMID: 36841895
- PMCID: PMC10011252
- DOI: 10.1007/s40123-023-00688-y
Cost-Utility Analysis of Deep Learning and Trained Human Graders for Diabetic Retinopathy Screening in a Nationwide Program
Abstract
Introduction: Deep learning (DL) for screening diabetic retinopathy (DR) has the potential to address limited healthcare resources by enabling expanded access to healthcare. However, there is still limited health economic evaluation, particularly in low- and middle-income countries, on this subject to aid decision-making for DL adoption.
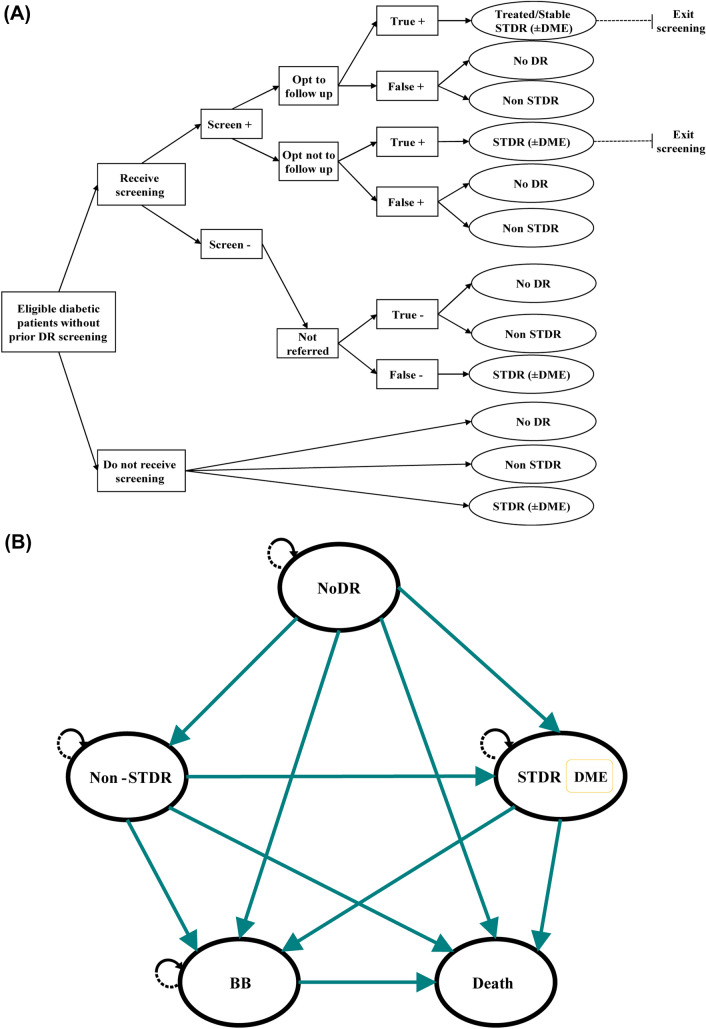
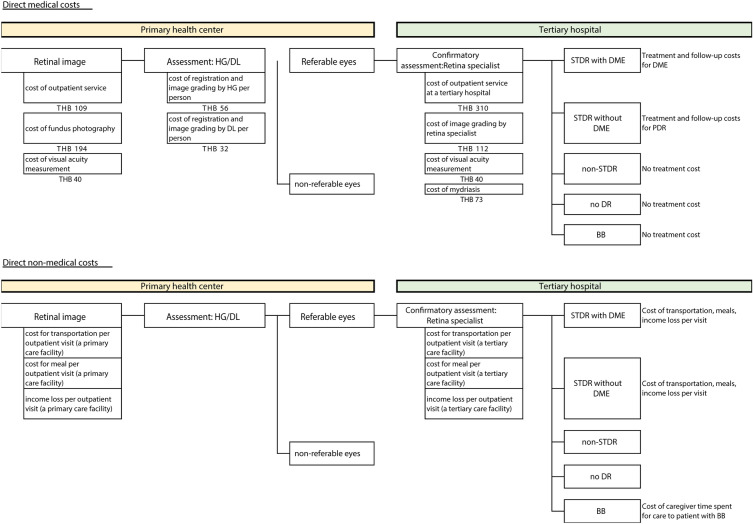
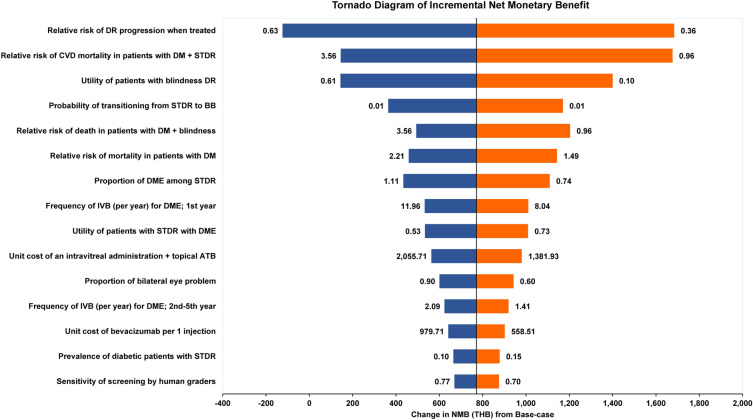
Methods: In the context of a middle-income country (MIC), using Thailand as a model, we constructed a decision tree-Markov hybrid model to estimate lifetime costs and outcomes of Thailand's national DR screening program via DL and trained human graders (HG). We calculated the incremental cost-effectiveness ratio (ICER) between the two strategies. Sensitivity analyses were performed to probe the influence of modeling parameters.
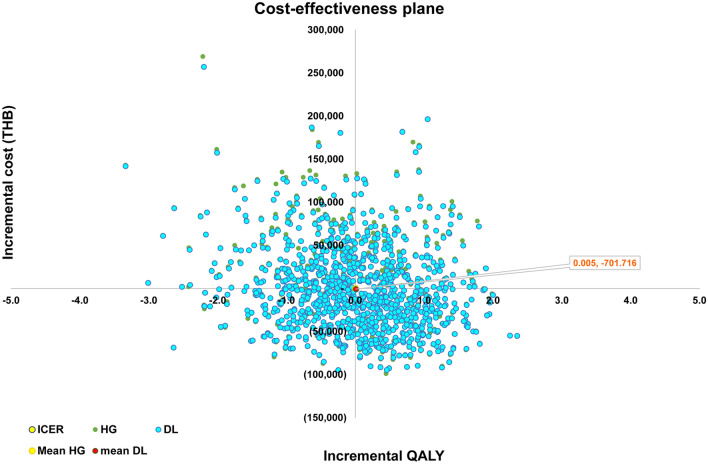
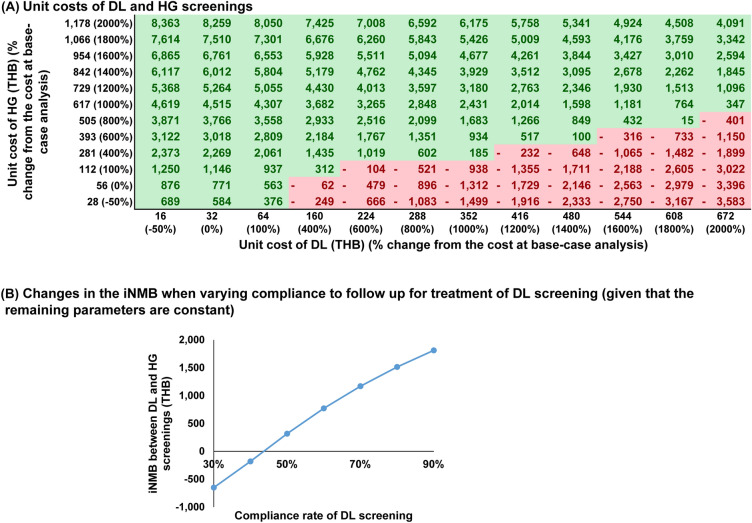
Results: From a societal perspective, screening with DL was associated with a reduction in costs of ~ US$ 2.70, similar quality-adjusted life-years (QALY) of + 0.0043, and an incremental net monetary benefit of ~ US$ 24.10 in the base case. In sensitivity analysis, DL remained cost-effective even with a price increase from US$ 1.00 to US$ 4.00 per patient at a Thai willingness-to-pay threshold of ~ US$ 4.997 per QALY gained. When further incorporating recent findings suggesting improved compliance to treatment referral with DL, our analysis models effectiveness benefits of ~ US$ 20 to US$ 50 depending on compliance.
Conclusion: DR screening using DL in an MIC using Thailand as a model may result in societal cost-savings and similar health outcomes compared with HG. This study may provide an economic rationale to expand DL-based DR screening in MICs as an alternative solution for limited availability of skilled human resources for primary screening, particularly in MICs with similar prevalence of diabetes and low compliance to referrals for treatment.
Keywords: Artificial intelligence; Cost-utility analysis; Diabetic retinopathy; Health economics; Public health.
© 2023. The Author(s).
Figures

References
-
- Heydon P, Egan C, Bolter L, Chambers R, Anderson J, Aldington S, et al. Prospective evaluation of an artificial intelligence-enabled algorithm for automated diabetic retinopathy screening of 30 000 patients. Br J Ophthalmol. 2021;105:723–728. doi: 10.1136/bjophthalmol-2020-316594. - DOI - PMC - PubMed
-
- Beede E, Baylor E, Hersch F, Iurchenko A, Wilcox L, Ruamviboonsuk P, et al. A human-centered evaluation of a deep learning system deployed in clinics for the detection of diabetic retinopathy. In: Proc 2020 CHI conf hum factors comput syst. New York: ACM; 2020. p. 1–12
LinkOut - more resources
Full Text Sources
