

Monitoring of pulmonary involvement in critically ill COVID-19 patients - should lung ultrasound be preferred over CT?
- PMID: 36842163
- PMCID: PMC9968403
- DOI: 10.1186/s13089-022-00299-x
Monitoring of pulmonary involvement in critically ill COVID-19 patients - should lung ultrasound be preferred over CT?
Abstract
Background: It is unclear if relevant changes in pulmonary involvement in critically ill COVID-19 patients can be reliably detected by the CT severity score (CTSS) and lung ultrasound score (LUSS), or if these changes have prognostic implications. In addition, it has been argued that adding pleural abnormalities to the LUSS could improve its prognostic value. The objective of this study was to compare LUSS and CTSS for the monitoring of COVID-19 pulmonary involvement through: first, establishing the correlation of LUSS (± pleural abnormalities) and CTSS throughout admission; second, assessing agreement and measurement error between raters for LUSS, pleural abnormalities, and CTSS; third, evaluating the association of the LUSS (± pleural abnormalities) and CTSS with mortality at different timepoints.
Methods: This is a prospective, observational study, conducted during the second COVID-19 wave at the AmsterdamUMC, location VUmc. Adult COVID-19 ICU patients were prospectively included when a CT or a 12-zone LUS was performed at admission or at weekly intervals according to local protocol. Patients were followed 90 days or until death. We calculated the: (1) Correlation of the LUSS (± pleural abnormalities) and CTSS throughout admission with mixed models; (2) Intra-class correlation coefficients (ICCs) and smallest detectable changes (SDCs) between raters; (3) Association between the LUSS (± pleural abnormalities) and CTSS with mixed models.
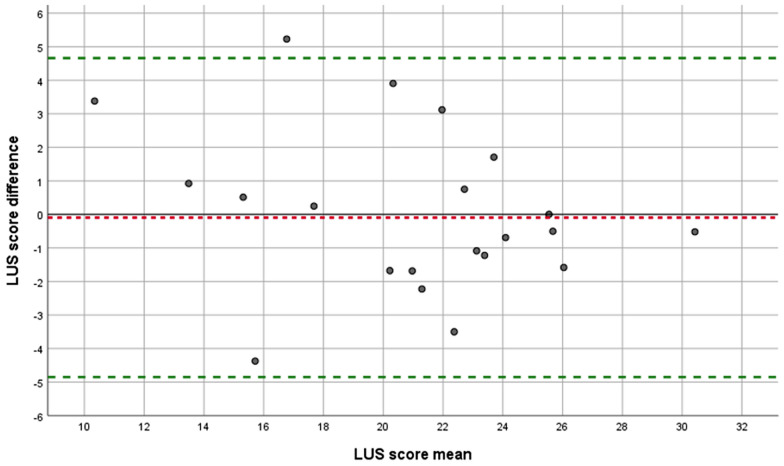
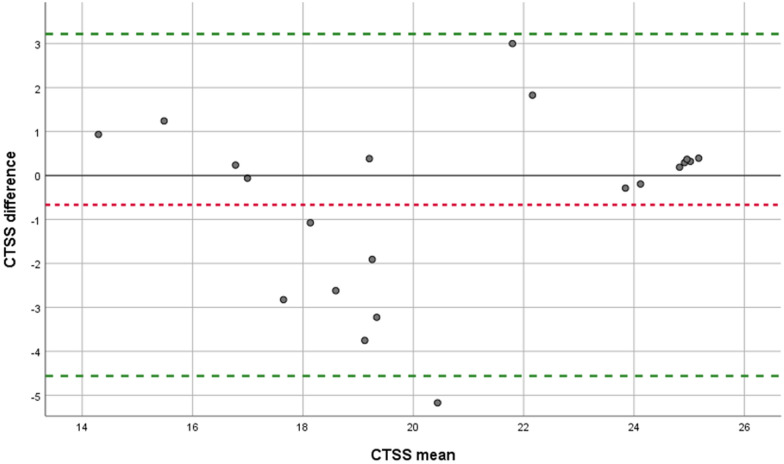
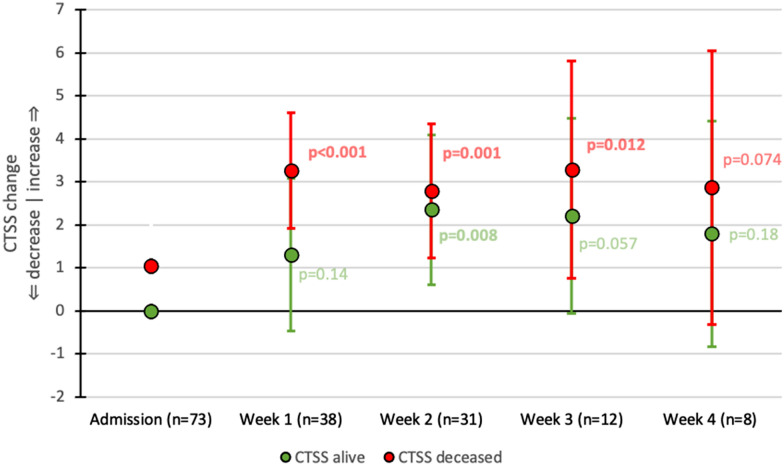
Results: 82 consecutive patients were included. Correlation between LUSS and CTSS was 0.45 (95% CI 0.31-0.59). ICCs for LUSS, pleural abnormalities, and CTSS were 0.88 (95% CI 0.73-0.95), 0.94 (95% CI 0.90-0.96), and 0.84 (95% CI 0.65-0.93), with SDCs of 4.8, 1.4, and 3.9. The LUSS was associated with mortality in week 2, with a score difference between patients who survived or died greater than its SDC. Addition of pleural abnormalities was not beneficial. The CTSS was associated with mortality only in week 1, but with a score difference less than its SDC.
Conclusions: LUSS correlated with CTSS throughout ICU admission but performed similar or better at agreement between raters and mortality prognostication. Given the benefits of LUS over CT, it should be preferred as initial monitoring tool.
Keywords: COVID-19; Computed tomography; Lung ultrasound; Monitoring; Mortality; Point-of-cafe ultrasound.
© 2023. The Author(s).
Conflict of interest statement
The authors have no conflict of interest nor any financial disclosures.
Figures


References
-
- Use of chest imaging in COVID-19. https://www.who.int/publications-detail-redirect/use-of-chest-imaging-in.... Accessed 13 Jun 2020.
LinkOut - more resources
Full Text Sources
Miscellaneous