

Imaging of lumpectomy surface with large field-of-view confocal laser scanning microscopy 'Histolog® scanner' for breast margin assessment in comparison with conventional specimen radiography
- PMID: 36842192
- PMCID: PMC9988675
- DOI: 10.1016/j.breast.2023.02.010
Imaging of lumpectomy surface with large field-of-view confocal laser scanning microscopy 'Histolog® scanner' for breast margin assessment in comparison with conventional specimen radiography
Abstract
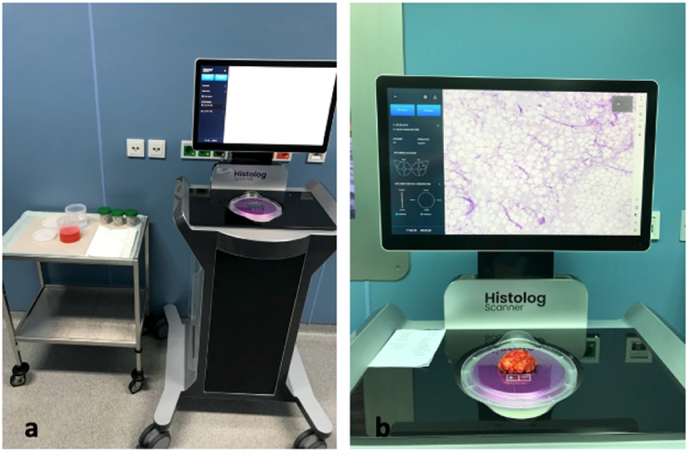
Purpose: The Histolog® Scanner (SamanTree Medical SA, Lausanne, Switzerland) is a large field-of-view confocal laser scanning microscope designed to allow intraoperative margin assessment by the production of histological images ready for assessment in the operating room. We evaluated the feasibility and the performance of the Histolog® Scanner (HS) to correctly identify infiltrated margins in clinical practice of lumpectomy specimens. It was extrapolated if the utilization of the HS has the potential to reduce infiltrated margins and therefore reduce re-operation rates in patients undergoing breast conserving surgery (BCS) due to a primarily diagnosed breast cancer including ductal carcinoma in situ.
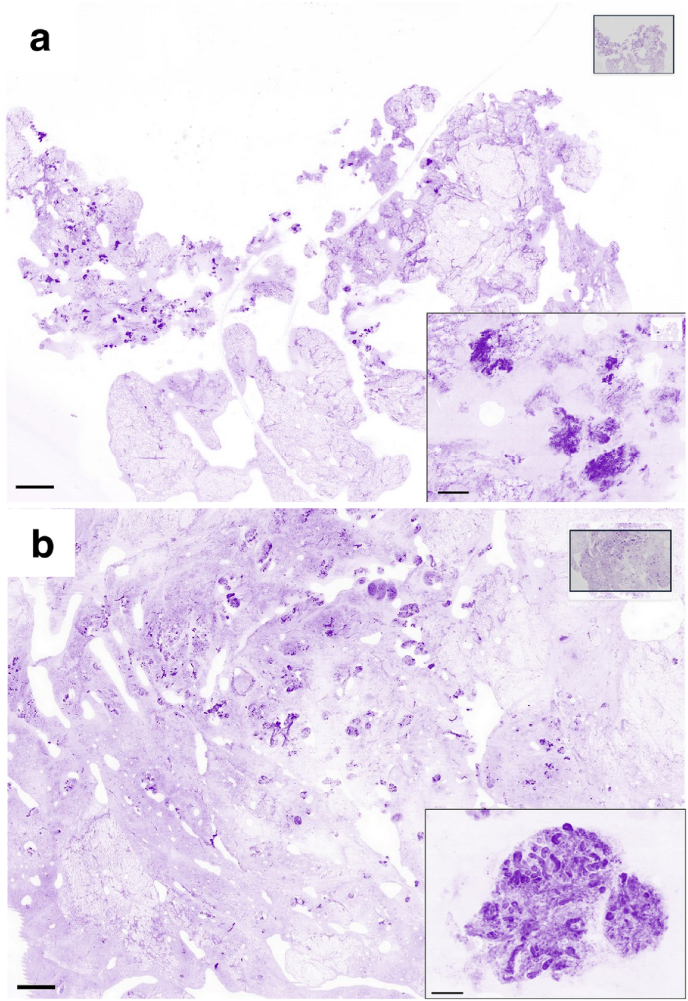
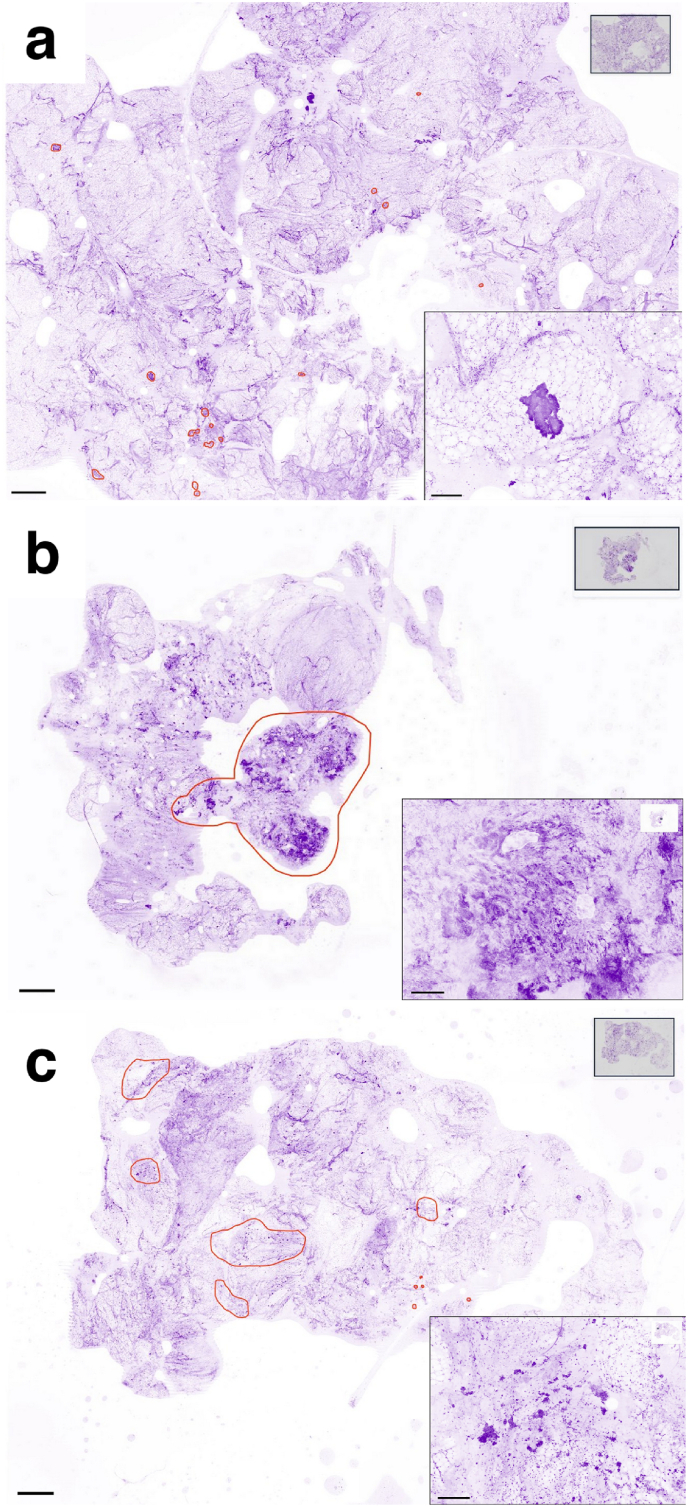
Methods: This is a single-center, prospective, non-interventional, diagnostic pilot study including 50 consecutive patients receiving BCS. The complete surface of the specimen was scanned using the HS intraoperatively. The surgery and the intraoperative margin assessment of the specimen was performed according to the clinical routine consisting of conventional specimen radiography as well as the clinical impression of the surgeon. Three surgeons and an experienced pathologist assessed the scans produced by the HS for cancer cells on the surface. The potential of the HS to correctly identify involved margins was compared to the results of the conventional specimen radiography alone as well as the clinical routine. The histopathological report served as the gold standard.
Results: 50 specimens corresponding to 300 surfaces were scanned by the HS. The mean sensitivity of the surgeons to identify involved margins with the HS was 37.5% ± 5.6%, the specificity was 75.2% ± 13.0%. The assessment of resection margins by the pathologist resulted in a sensitivity of 37.5% and a specificity of 81.0%, while the local clinical routine resulted in a sensitivity of 37.5% and a specificity of 78.2%.
Conclusion: Acquisition of high-resolution histological images using the HS was feasible in clinical practice. Sensitivity and specificity were comparable to clinical routine. With more specific training and experience on image interpretation and acquisition, the HS may have the potential to enable more accuracy in the margin assessment of BCS specimens.
Keywords: Breast cancer; Breast conserving surgery; Confocal microscopy; Conventional specimen radiography; Fresh tissue imaging; Margin assessment.
Copyright © 2023 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Prof. Dr. Michael Golatta reports financial support was provided by SamanTree Medical SA. Prof. Michael Lux reports financial support was provided by SamanTree Medical SA.
Figures
References
-
- Rojas K., Stuckey A. Breast cancer epidemiology and risk factors. Clin Obstet Gynecol. 2016;59:651–67210. 1097/grf.0000000000000239. - PubMed
-
- Hofvind S., Holen Å., Aas T., Roman M., Sebuødegård S., Akslen L.A. Women treated with breast conserving surgery do better than those with mastectomy independent of detection mode, prognostic and predictive tumor characteristics. Eur J Surg Oncol. 2015;41:1417–142210. 1016/j.ejso.2015.07.002. - PubMed
-
- Lagendijk M., van Maaren M.C., Saadatmand S., Strobbe L.J.A., Poortmans P.M.P., Koppert L.B., Tilanus-Linthorst M.M.A., Siesling S. Breast conserving therapy and mastectomy revisited: breast cancer-specific survival and the influence of prognostic factors in 129,692 patients. Int J Cancer. 2018;142:165–17510. 1002/ijc.31034. - PubMed
-
- Rosenberg S.M., Dominici L.S., Gelber S., Poorvu P.D., Ruddy K.J., Wong J.S., Tamimi R.M., Schapira L., Come S., Peppercorn J.M., Borges V.F., Partridge A.H. Association of breast cancer surgery with quality of life and psychosocial well-being in young breast cancer survivors. JAMA Surg. 2020;155:1035–104210. 1001/jamasurg.2020.3325. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
