

Clinical features, risk factors, diagnosis, and treatment of trimethoprim-sulfamethoxazole-induced hypoglycemia
- PMID: 36843590
- PMCID: PMC9944732
- DOI: 10.3389/fendo.2023.1059522
Clinical features, risk factors, diagnosis, and treatment of trimethoprim-sulfamethoxazole-induced hypoglycemia
Abstract
Objective: Hypoglycemia is a sporadic and serious adverse reaction of trimethoprim-sulfamethoxazole (TMP-SMX) due to its sulfonylurea-like effect. This study explored the clinical characteristics, risk factors, treatment, and prognosis of TMP-SMX-induced hypoglycemia.
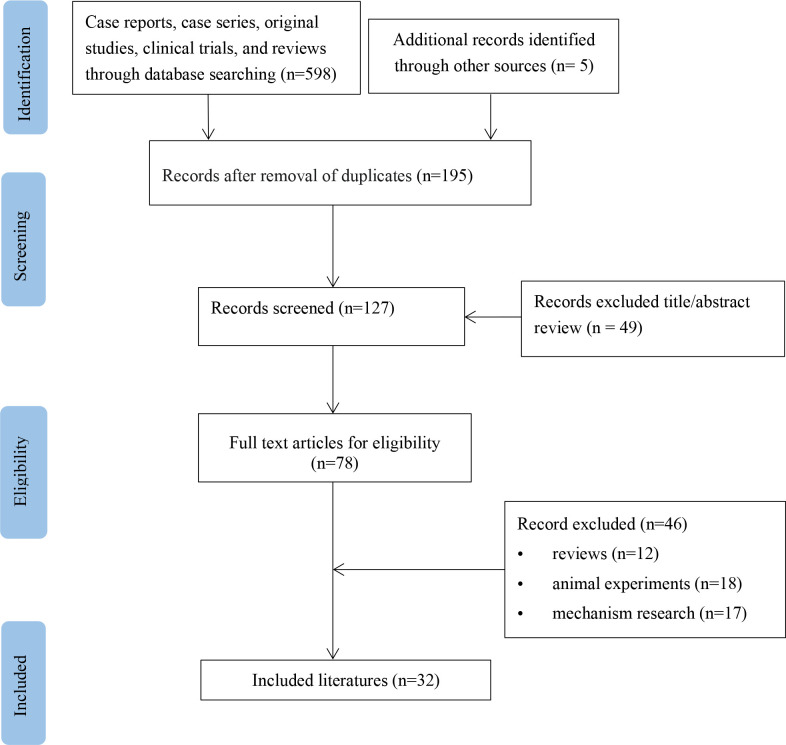
Methods: Case reports and series of TMP-SMX-induced hypoglycemia were systematically searched using Chinese and English databases. Primary patient and clinical information were extracted for analysis.
Results: A total of 34 patients were reported from 31 studies (16 males and 18 females). The patients had a median age of 64 years (range 0.4-91), and 75.8% had renal dysfunction. The median duration of a hypoglycemic episode was six days (range 1-20), and the median minimum glucose was 28.8 mg/dL (range 12-60). Thirty-two patients (97.0%) showed neuroglycopenic symptoms, with consciousness disturbance (30.3%) and seizure (24.2%), sweating (18.2%), confusion (15.2%), asthenia (12.1%) being the most common symptoms. Fifteen patients (44.1%) had elevated serum insulin levels, with a median of 31.8 μU/mL (range 3-115.3). C-peptide increased in 13 patients (38.2%), with a median of 7.7 ng/mL (range 2.2-20). Complete recovery from symptoms occurred in 88.2% of patients without sequelae. The duration of hypoglycemia symptoms was 8 hours to 47 days after the intervention. Interventions included discontinuation of TMP-SMX, intravenous glucose, glucagon, and octreotide.
Conclusion: Hypoglycemia is a rare and serious adverse effect of TMP-SMX. Physicians should be aware of this potential adverse effect, especially in patients with renal insufficiency, increased drug doses, and malnutrition.
Keywords: hypoglycemia; neuroglycopenic symptoms; pneumocystis pneumonia; seizure; trimethoprim-sulfamethoxazole.
Copyright © 2023 Wang, Fang, Li and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Hypoglycemia secondary to trimethoprim/sulfamethoxazole administration in a renal transplant patient.Ann Pharmacother. 1993 Mar;27(3):304-6. doi: 10.1177/106002809302700309. Ann Pharmacother. 1993. PMID: 8453166 Review.
-
Trimethoprim-sulfamethoxazole-induced refractory hypoglycaemia successfully treated with octreotide.BMJ Case Rep. 2021 May 7;14(5):e240232. doi: 10.1136/bcr-2020-240232. BMJ Case Rep. 2021. PMID: 33962920 Free PMC article.
-
Trimethoprim/sulfamethoxazole-induced hypoglycemia in a patient with acute renal failure.Ann Pharmacother. 1997 Jun;31(6):727-32. doi: 10.1177/106002809703100611. Ann Pharmacother. 1997. PMID: 9184713
-
Renal Insufficiency in Concert with Renin-angiotensin-aldosterone Inhibition Is a Major Risk Factor for Hyperkalemia Associated with Low-dose Trimethoprim-sulfamethoxazole in Adults.Intern Med. 2016;55(5):467-71. doi: 10.2169/internalmedicine.55.5697. Epub 2016 Mar 1. Intern Med. 2016. PMID: 26935365
-
Analysis of the Clinical Characteristics of Hyponatremia Induced by Trimethoprim/Sulfamethoxazole.Pharmacology. 2022;107(7-8):351-358. doi: 10.1159/000523824. Epub 2022 Apr 5. Pharmacology. 2022. PMID: 35381593 Free PMC article. Review.
Cited by
-
Triple therapy for Helicobacter pylori eradication and the risk of hypoglycemia in patients with diabetes: a population-based cohort study.BMC Public Health. 2023 Sep 12;23(1):1772. doi: 10.1186/s12889-023-16689-2. BMC Public Health. 2023. PMID: 37700268 Free PMC article.
-
Transplant endocrinology.Med J Armed Forces India. 2023 Nov-Dec;79(6):651-656. doi: 10.1016/j.mjafi.2023.08.017. Epub 2023 Sep 12. Med J Armed Forces India. 2023. PMID: 37981924 Free PMC article. Review.
-
Evaluation of Adverse Events Associated with the Sulfamethoxazole/Trimethoprim Combination Drug.J Clin Med. 2025 Jul 8;14(14):4819. doi: 10.3390/jcm14144819. J Clin Med. 2025. PMID: 40725512 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical