

Abnormal vibration perception threshold alters the gait features in type 2 diabetes mellitus patients
- PMID: 36844372
- PMCID: PMC9944365
- DOI: 10.3389/fendo.2022.1092764
Abnormal vibration perception threshold alters the gait features in type 2 diabetes mellitus patients
Abstract
Objective: It is generally believed that gait characteristics of diabetic neuropathic patients differ from those of non-diabetic ones. However, it is still unclear how the abnormal foot sensation influences the gait during walking in type 2 diabetes mellitus (T2DM). For the purpose of gaining a better insight into the alterations of detailed gait parameters and figuring out important aspects in the gait indexes by peripheral neuropathy in elder T2DM patients, we compared the gait features in participants with normal glucose tolerance (NGT) controls and diabetic individuals complicated by peripheral neuropathy or not.
Subjects and methods: Gait parameters were observed during the 10-m walk on flat land among different conditions of diabetes in 1,741 participants from three clinical centers. Subjects were divided into four groups: persons with NGT were taken as the control group; patients with T2DM included three subgroups: DM control (no chronic complications), DM-DPN (DM complicated by only peripheral neuropathy), and DM-DPN+LEAD (DM complicated by both neuropathy and artery disease). The clinical characteristics and gait parameters were assessed and compared among these four groups. Analyses of variance were employed to verify possible differences of gait parameters between groups and conditions. Stepwise multivariate regression analysis was performed to reveal possible predictors of gait deficits. Receiver operating characteristic (ROC) curve analysis was employed to find any discriminatory power of diabetic peripheral neuropathy (DPN) for the step time.
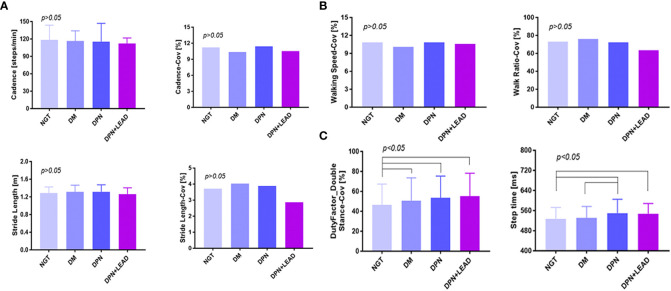
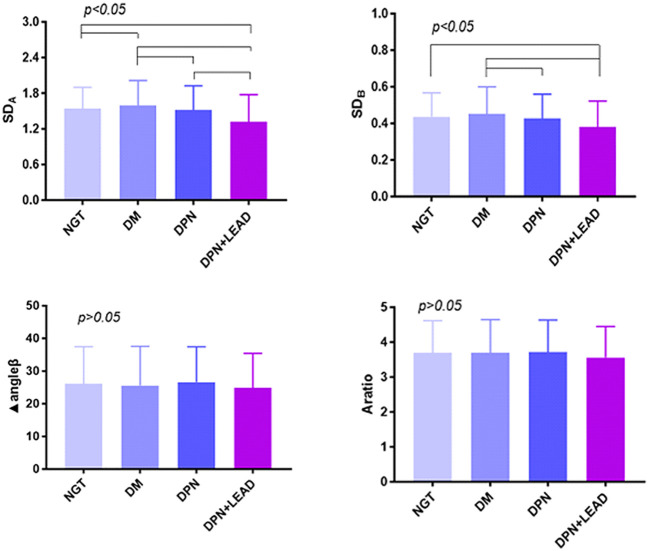
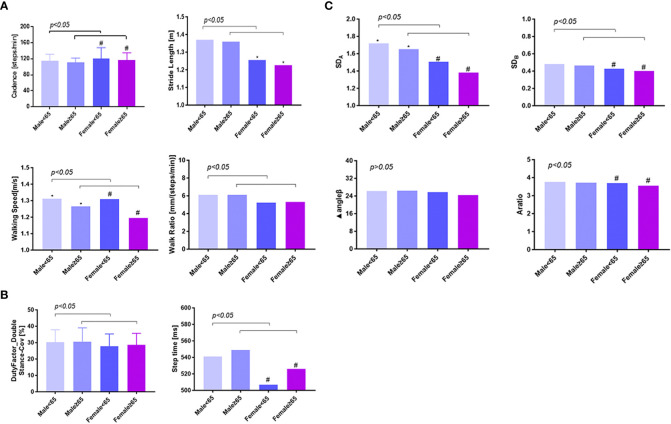
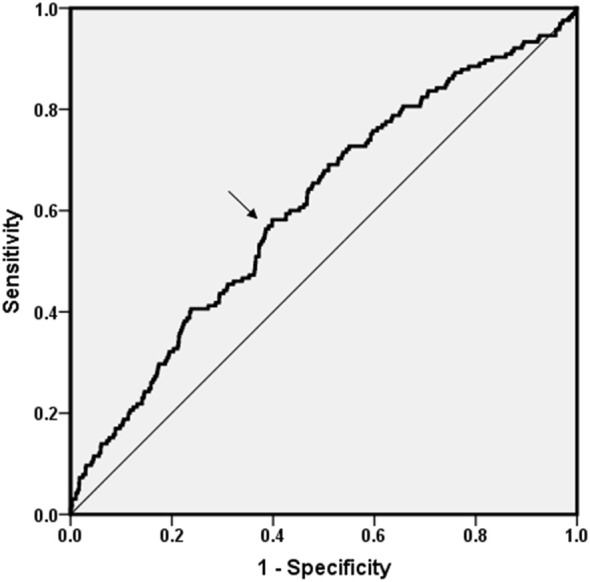
Results: In participants burdened with DPN, whether complicated by lower extremity arterial disease (LEAD) or not, step time increased sharply (p < 0.05). Stepwise multivariate regression models showed that independent variables of gait abnormality were sex, age, leg length, vibration perception threshold (VPT), and ankle-brachial index (ABI) (p < 0.01). Meanwhile, VPT was a significant independent predictor of step time, spatiotemporal variability (SDA), and temporal variability (SDB) (p < 0.05). ROC curve analysis was explored to find the discriminatory power of DPN for the occurrence of increased step time. The area under the curve (AUC) value was 0.608 (95% CI: 0.562-0.654, p < 0.01), and the cutoff point was 538.41 ms accompanied by a higher VPT. A significant positive association was observed between increased step time and the highest VPT group [odds ratio (OR) = 1.83, 95% CI: 1.32-2.55, p< 0.01]. In female patients, this OR value elevated to 2.16 (95% CI: 1.25-3.73, p< 0.01).
Conclusions: In addition to sex, age, and leg length, VPT was a distinct factor that associated with altered gait parameters. DPN is associated with increased step time, and the step time increases with worsening VPT in type 2 diabetes.
Keywords: complication; diabetic; diabetic peripheral neuropathy; gait; type 2 diabetes; vibrating perception threshold.
Copyright © 2023 Dong, Hu, Xu, Zeng, Shen, Esser, Dawes and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer JW is currently organizing a Research Topic with the author FL.
Figures
References
-
- Almurdhi MM, Brown SJ, Bowling FL, Boulton AJM, Jeziorska M, et al. Altered walking strategy and increased unsteadiness in participants with impaired glucose tolerance and type 2 diabetes relates to small-fibre neuropathy but not vitamin d deficiency. Diabetes Med (2017) 34(6):839–45. doi: 10.1111/dme.13316 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical