

doi: 10.1109/ismr48331.2020.9312937.
Epub 2021 Jan 11.
Computational Optimization of Notch Spacing for a Transnasal Ear Endoscopy Continuum Robot
Affiliations
- PMID: 36844884
- PMCID: PMC9948123
- DOI: 10.1109/ismr48331.2020.9312937
Item in Clipboard
Computational Optimization of Notch Spacing for a Transnasal Ear Endoscopy Continuum Robot
Int Symp Med Robot.
2020 Nov.
Abstract
This paper presents a computational framework to optimize the visual coverage attainable by a notched-tube continuum robotic endoscope inside the middle ear cavity. Our framework combines anatomically-accurate geometric (mesh) models of the middle ear with a sampling-based motion planning algorithm (RRT) and a ray-casting procedure to quantify what regions of the middle ear can be accessed and visualized by the endoscope. To demonstrate the use of this framework, we run computer simulations to investigate the effect of varying the distance between each pair of consecutive flexure elements (i.e., notches) in our robotic endoscope.
Figures
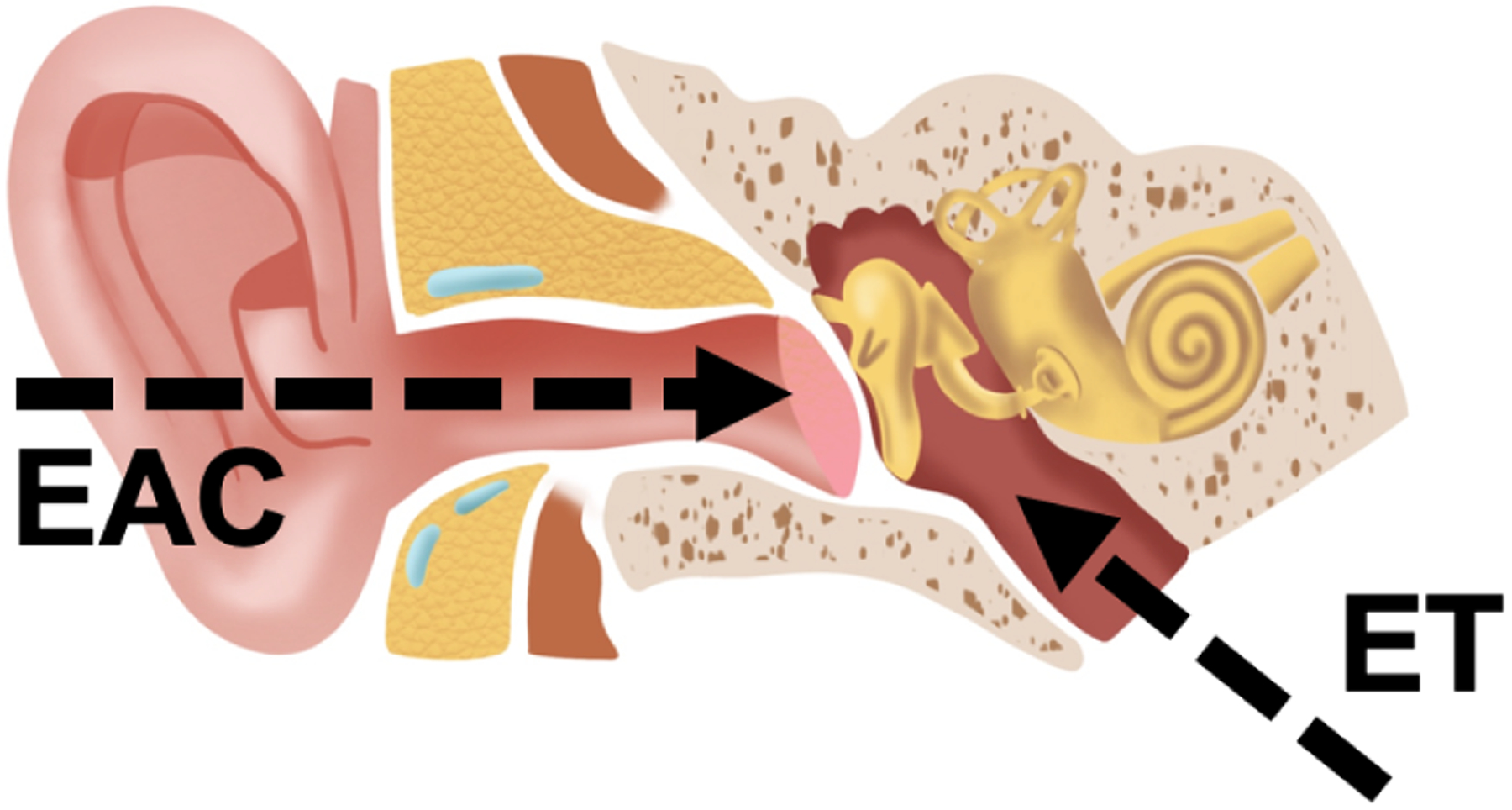
Anatomy of the human ear. Two natural orifices provide access to the middle ear cavity: the external ear canal (EAC) and the Eustachian tube (ET). To access the middle ear from the EAC, surgeons have to cut or lift the tympanic membrane. By contrast, accessing the middle ear by way of the ET does not require the disruption of any tissue.
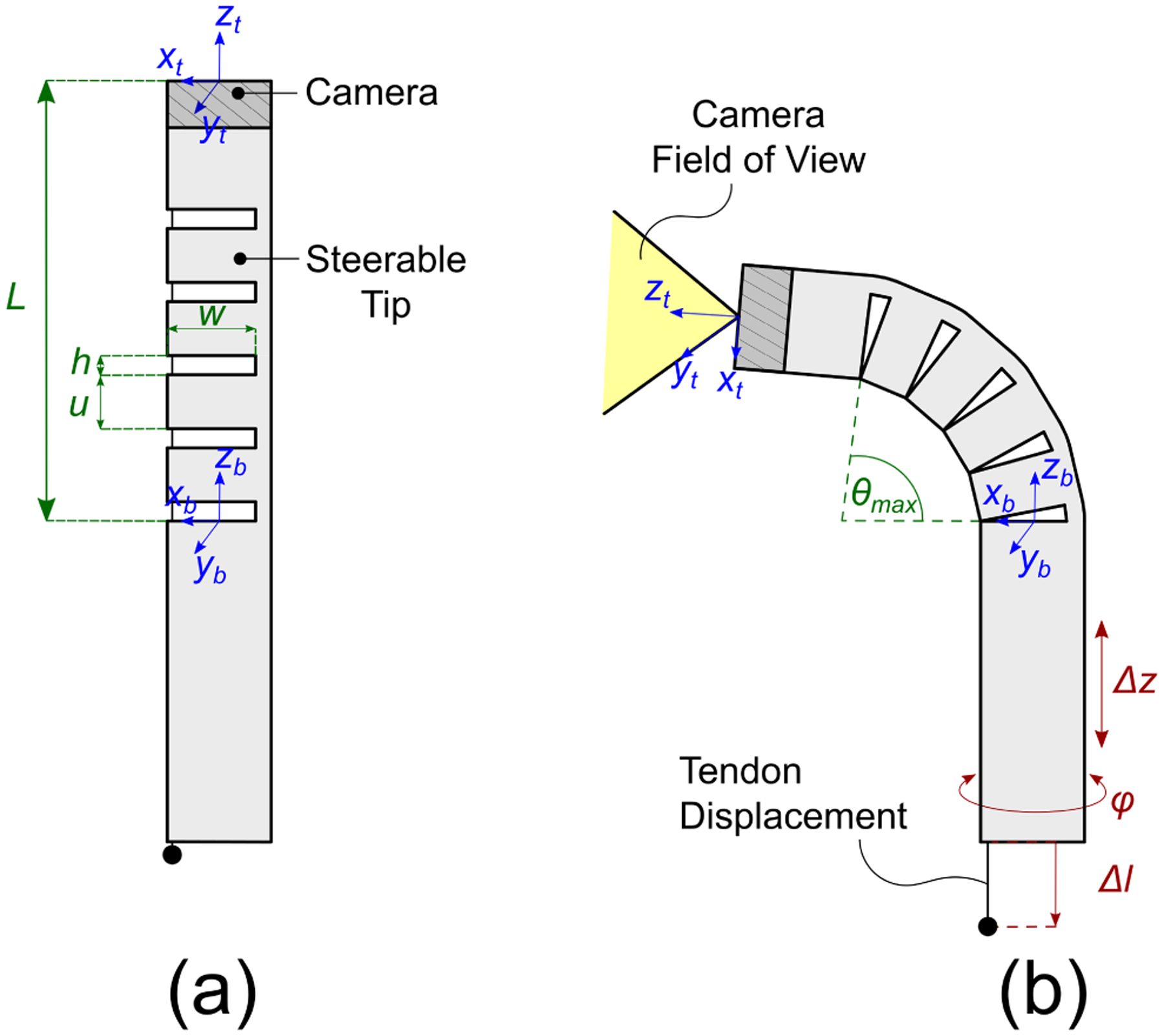
Robotic endoscope concept: a digital chip-tip camera is installed at the tip of a Nickel-Titanium (Nitinol) tube. Asymmetric notches are cut in the body of the tube, creating a compliant section that can be articulated by pulling a single tendon attached at the tip of the robot. (a) Robot in its base ”straight” configuration; the design parameters of the notched section include the number of notches n, the notch height h, the notch width w, and the spacing u between each pair of notches; (b) The robot is equipped with a total of three degrees of freedom, namely axial translation (Δz), axial rotation (φ) and tendon displacement (Δl).
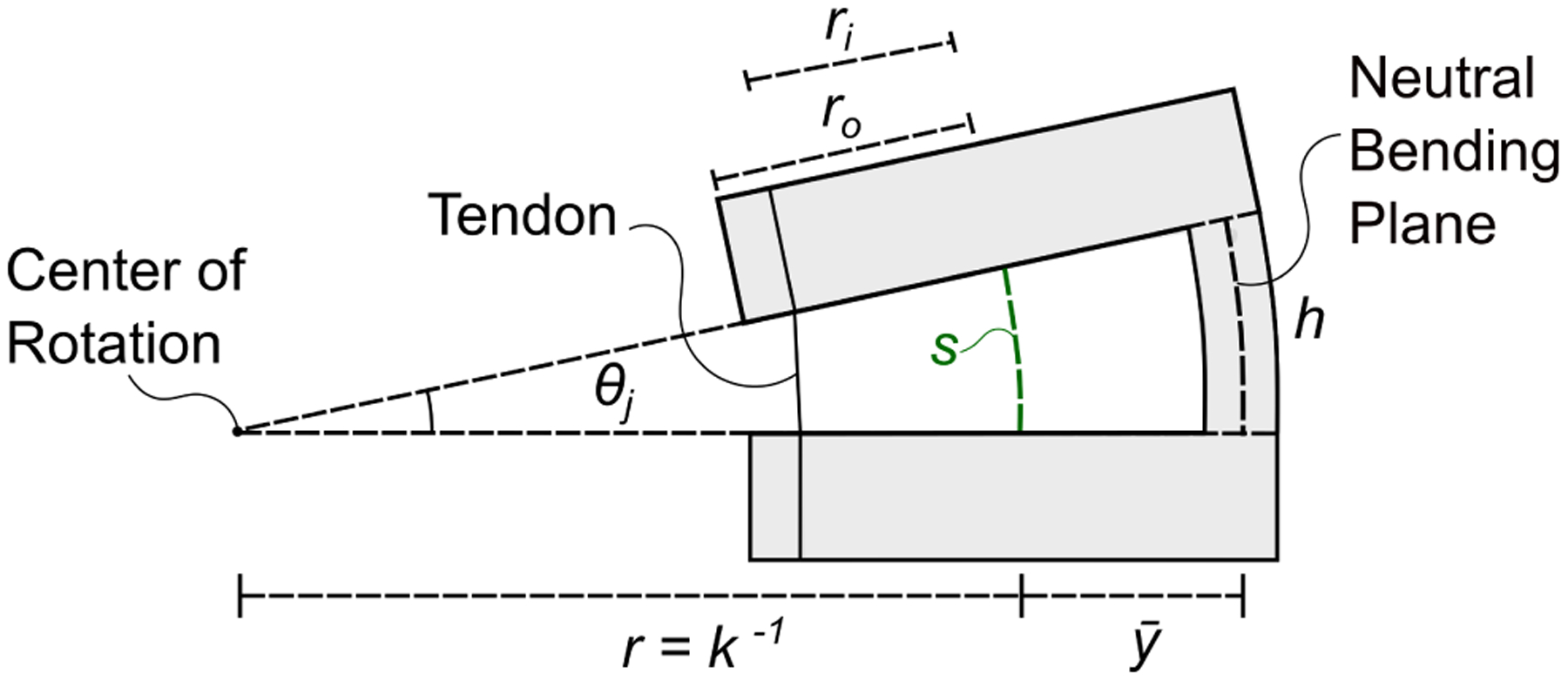
Close-up view of a single notch. Cutting asymmetric notches offsets the neutral bending plane of the tube, i.e. the plane which experiences no strain during bending, which is now located at a distance from the center line of the tube. The value of can be calculated using the equations in [20], [21]. Applying a tensile force on the tendon makes the notch bend in the shape of a constant-curvature arc characterized by an arc length s and a curvature κ. Another important geometric characteristic of a notch is the height h (which in this figure is measured by the neutral bending axis). Finally, ro and ri are the outer and inner radius of the Nitinol tube.
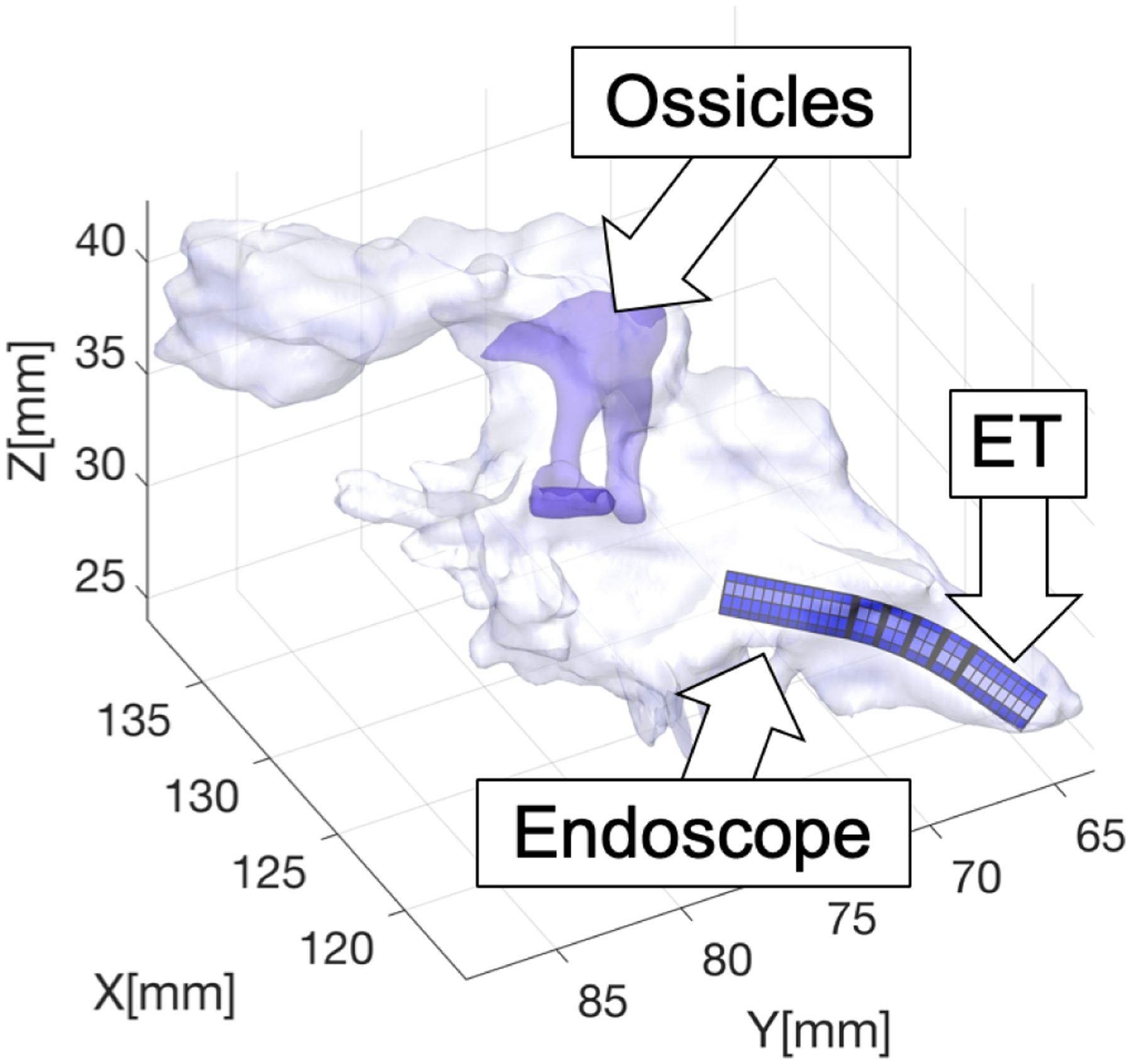
Simulation of trans-Eustachian middle ear endoscopy.
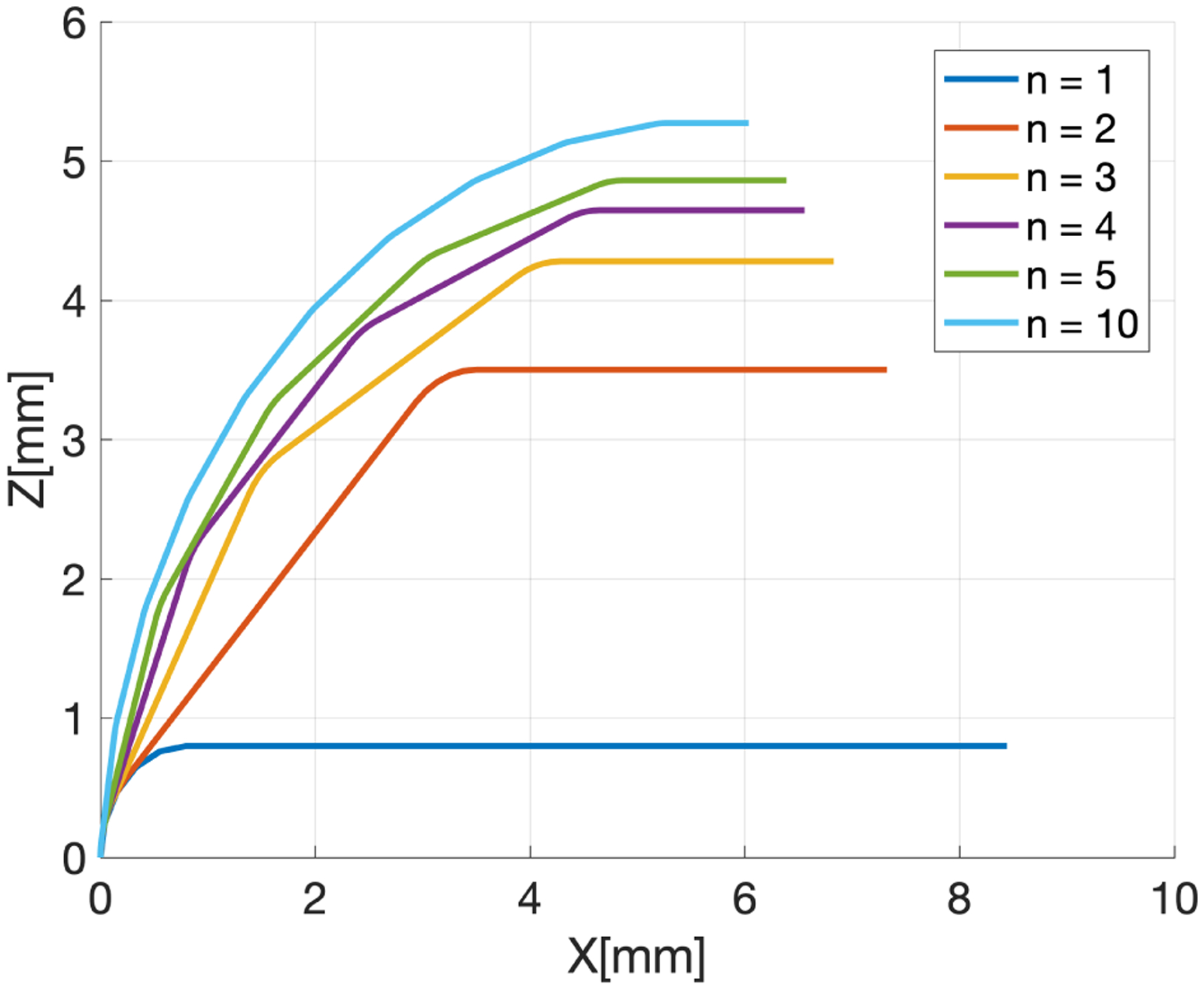
Effect of the number of notches n on the endoscope bending. The different lines represent the backbone of the endoscope at full bending. No rotation is applied, therefore bending occurs entirely in the XZ plane. The straight sections have length u, while the flexure elements have length s (Eq. 3). To generate these lines, we imposed θmax = 90° and L = 10 mm.
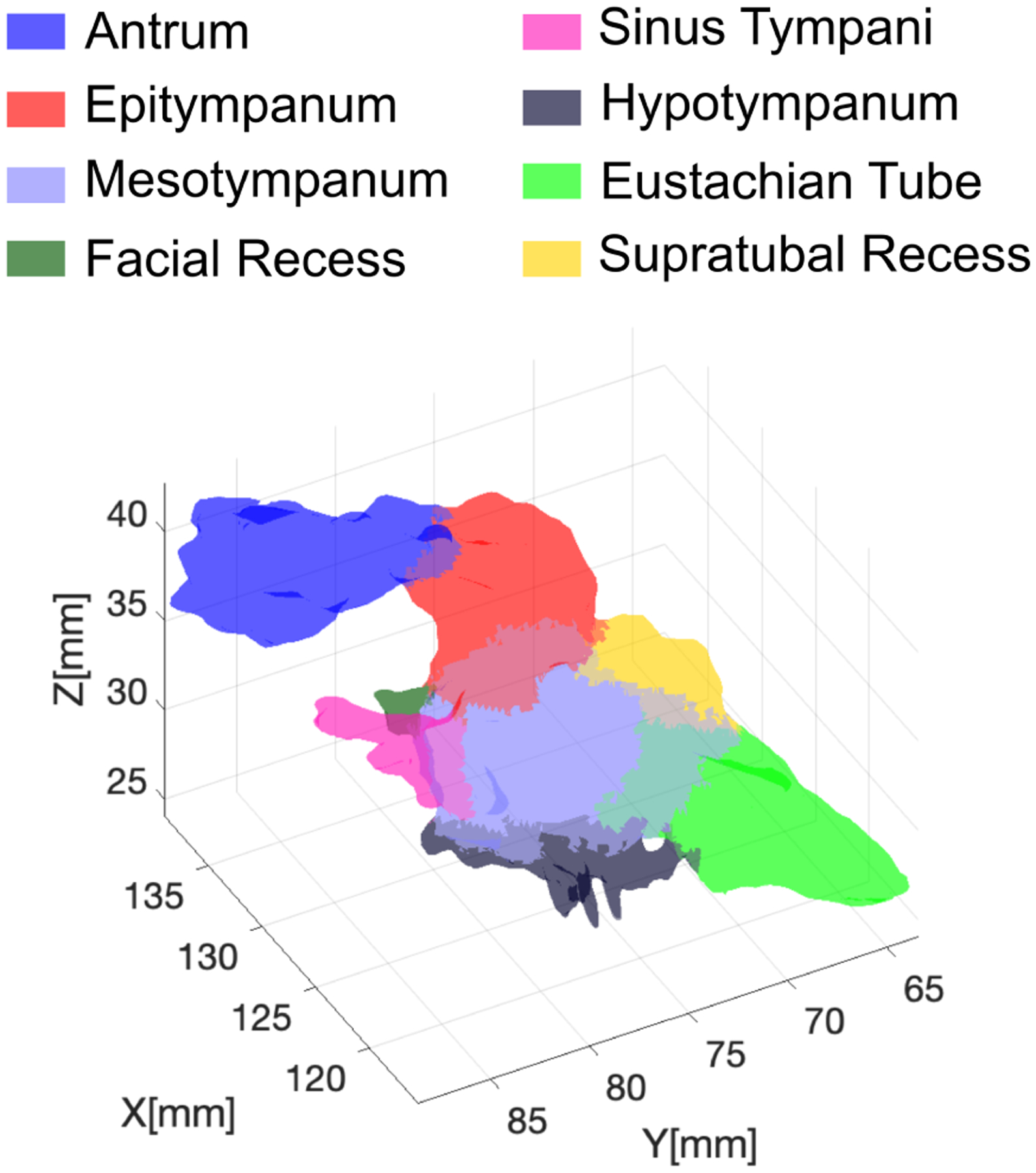
Geometric model of the ear highlighting different anatomical sub-regions.
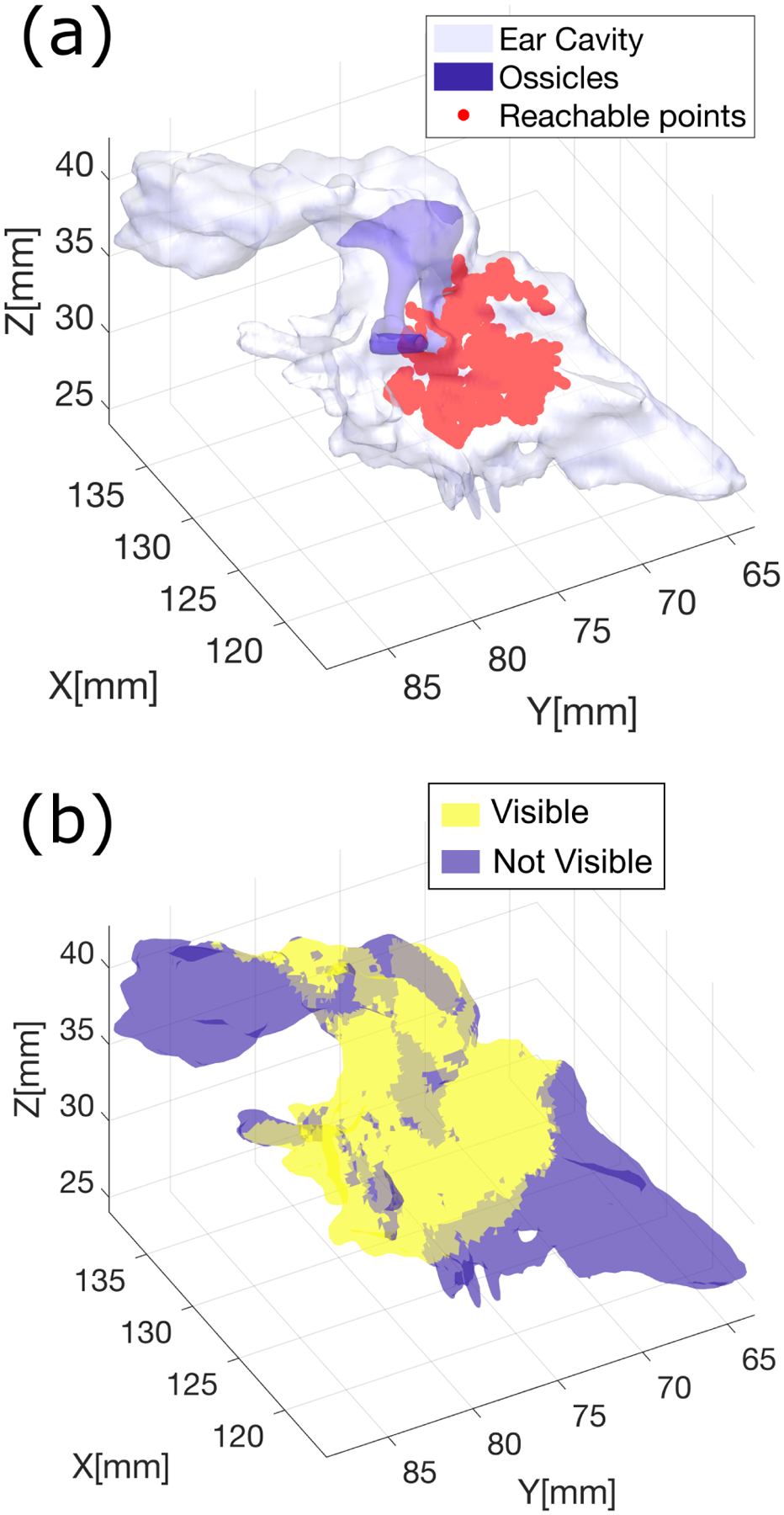
Visual coverage estimation: (a) Reachable points calculated via RRT; (b) Map showing visible regions within the ear.
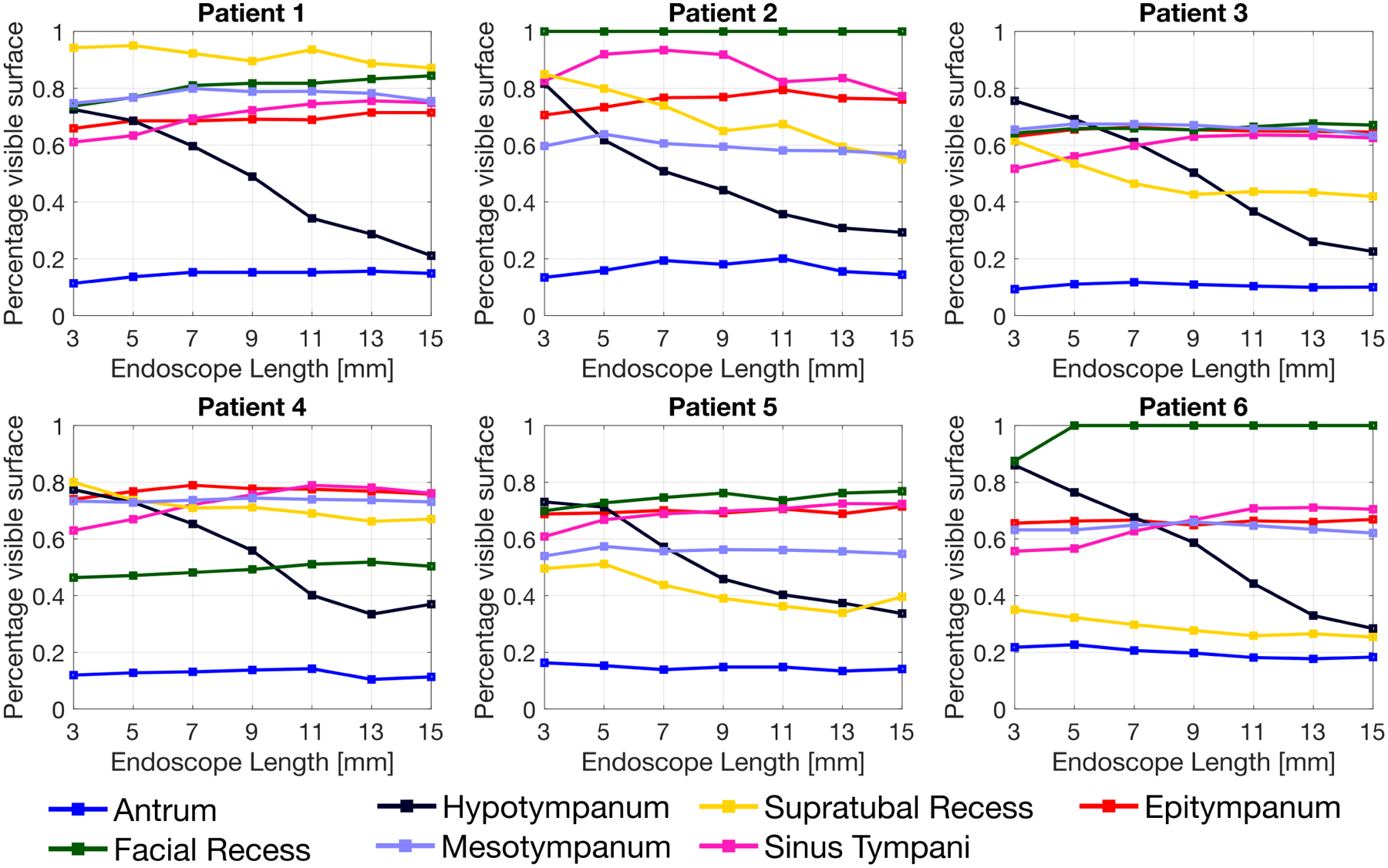
Simulation results. The visual coverage achieved by the endoscope in any given anatomical region is expressed as a percentage of the total surface in that region.
References
-
- French LC, Dietrich MS, and Labadie RF, “An estimate of the number of mastoidectomy procedures performed annually in the united states,” Ear, Nose & Throat Journal, vol. 87, no. 5, pp. 267–270, 2008. - PubMed
-
- Brackmann D, Shelton C, and Arriaga MA, Otologic Surgery. Elsevier Health Sciences, 2015.
-
- Crowson MG, Ramprasad VH, Chapurin N, Cunningham III CD, and Kaylie DM, “Cost analysis and outcomes of a second-look tympanoplasty-mastoidectomy strategy for cholesteatoma,” The Laryngoscope, vol. 126, no. 11, pp. 2574–2579, 2016. - PubMed
-
- Marchioni D, Valerini S, Mattioli F, Alicandri-Ciufelli M, and Presutti L, “Radiological assessment of the sinus tympani: temporal bone hrct analyses and surgically related findings,” Surgical and Radiologic Anatomy, vol. 37, no. 4, pp. 385–392, 2015. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources